Chronic nasal congestion, the constant condition of not being able to breathe through your nose, can be a major problem, interferes with sleep (often via sleep apnea), undermining one of the 4 pillars of health (sleep, diet, exercise and intellectual stimulation). Well, maybe a second one as well, since it is hard to function intellectually when you are sleepy all the time.
Chronic nasal congestion in kids is often due to allergy and associated ADENOID (located at the back of the throat) ENLARGEMENT. Adenoids can cause sleep apnea and pulmonary hypertension, ear infections and sinusitis.
If left untreated, the bones of the face don’t grow properly, and the constricted bony structures can lead to later problems. Nasal polyps can be a factor in nasal airflow blockage, and their removal may benefit the blockage.
If associated with sinusitis and aspirin (aspirin is rarely used in children anymore because if Reyes’ Syndrome) sensitivity, the combination is known as “sampters’ triad. Regrowth of the polyps is common and aspirin desensitization may be helpful.
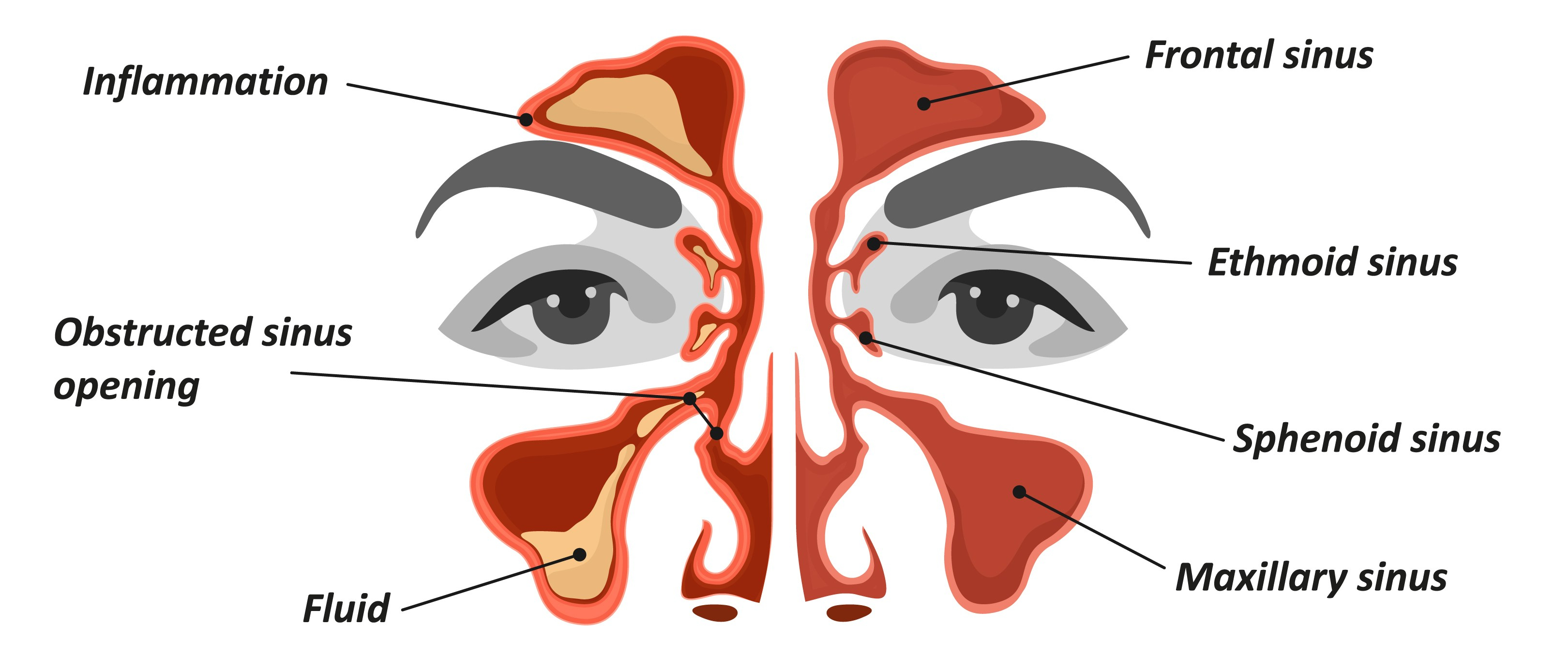
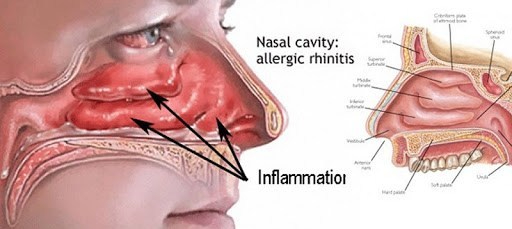
ALLERGIC RHINITIS is treated by avoidance, medication and desensitization. SINUSITIS can cause chronic nasal blockage. Both medical and surgical treatments are useful.
One-sided nasal blockage raises a red flag. One of my young patients had pushed a rock into his nose, which I then removed. Nasal polyps can be on one side, and can be removed, NASAL SEPTAL DEVIATION can cause one-sided nasal blockage, and if severe can be surgically corrected.
The nasal tissues are “erectile tissues” I have a nasal septal deviation to my left side. I SLEEP ON MY SIDE to CONTROL my SLEEP APNEA (more when I get to that subject, which certainly qualifies as a chronic problem), When I sleep on my right side, I don’t breathe as well since my “good side” is down and becomes study.
Those lucky people who breathe freely on both sides, and who sleep on their sides, may possibly be aware that the DOWN SIDE (my good side, above) blocks up. It seems that the nasal tissues are “erectile tissues” body wants to REST one side at a time, and the down side is easier, since gravity pools the blood there.
Nasal tissues are under the control of the autonomic nervous system, decongest (nasal passages are open) with the alarm (fight or flight, “sympathetic”) reaction, and do the opposite (tissues congest, nasal passages close) when the “parasympathetic” takes over after a meal, when you are “vegetating”. in front of the TV