My Mother had Tic Douloureux, the traditional name for Trigeminal Neuralgia. I remember her suddenly covering her face with her hand and grimacing, but this was only occasionally.
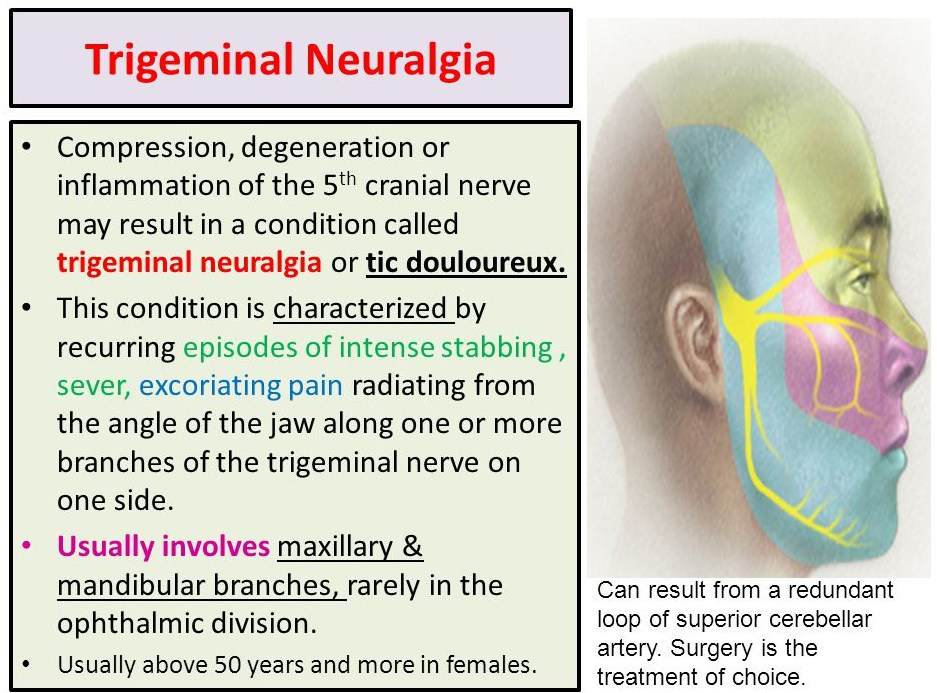
Compression, degeneration or inflammation of the 5th cranial nerve may result in a condition called trigeminal neuralgia or tic douloureux. This condition is characterized by recurring episodes of intense stabbing , sever, excoriating pain radiating from the angle of the jaw along one or more branches of the trigeminal nerve on one side. Usually involves maxillary & mandibular branches, rarely in the ophthalmic division. Usually above 50 years and more in females. Can result from a redundant loop of superior cerebellar artery. Surgery is the treatment of choice.
TD is not very common for “101 chronic conditions”, but it is the most common cause of chronic facial pain. It occurs in the FACIAL region supplied by the 5th cranial, or TRIGEMINAL nerve. This is about the area covered by your widely spread hand, pinkie on the nose, and the butt of the palm along the jawbone.
Brief shocking pain occurs in “PAROXYSMS” in the facial area, on ONE SIDE, and TRIGGERED by tooth brushing, touching the face, or even by the blowing of the wind. This description is so typical and specific as to be “pathognomonic”, and can be diagnosed over the telephone.
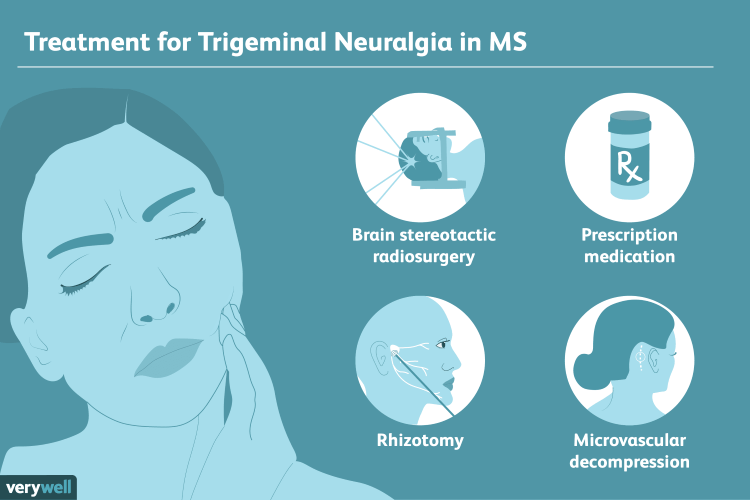
Variants can give continuous pain, or occur on both sides, but the “classical” variety is most common. You should contact your Doctor, since some cases are caused by Multiple Sclerosis or a tumor. Effective medications are available, such as carbamazepine.
TD can be familial, but is often caused by compression of a nearby artery, and “decompression” is currently the most effective surgical treatment. It is one of the few “chronic 101” conditions not to be substantially prevented or helped by our old standbys, sleep, diet and exercise.
That being said, it is sometimes helped by exercise, and almost never occurs during sleep. The August 20, 2020 New England Journal of Medicine Has an excellent Review article, which will be appended to this posting.
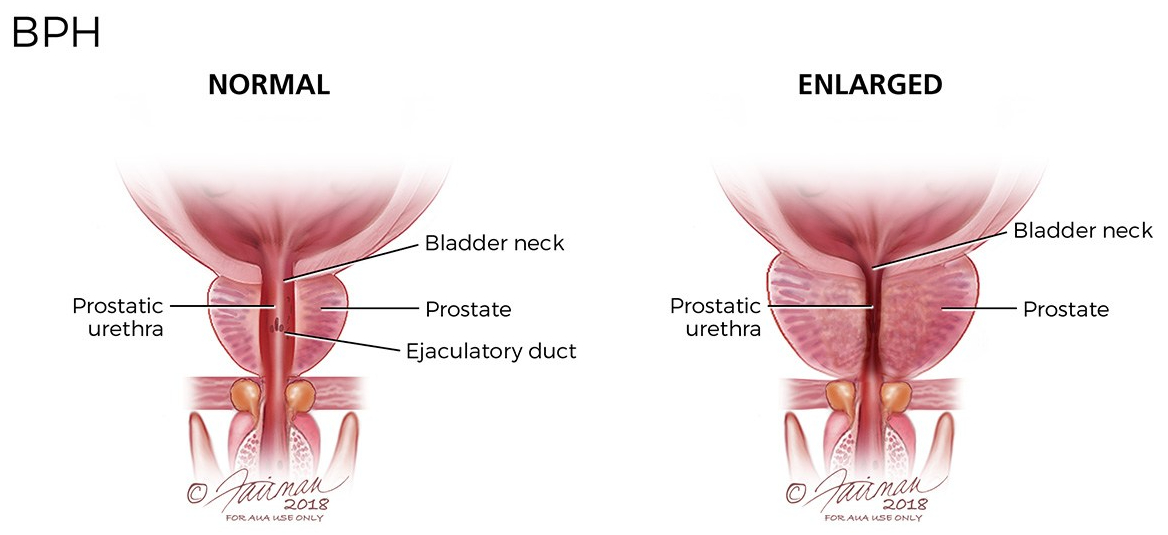
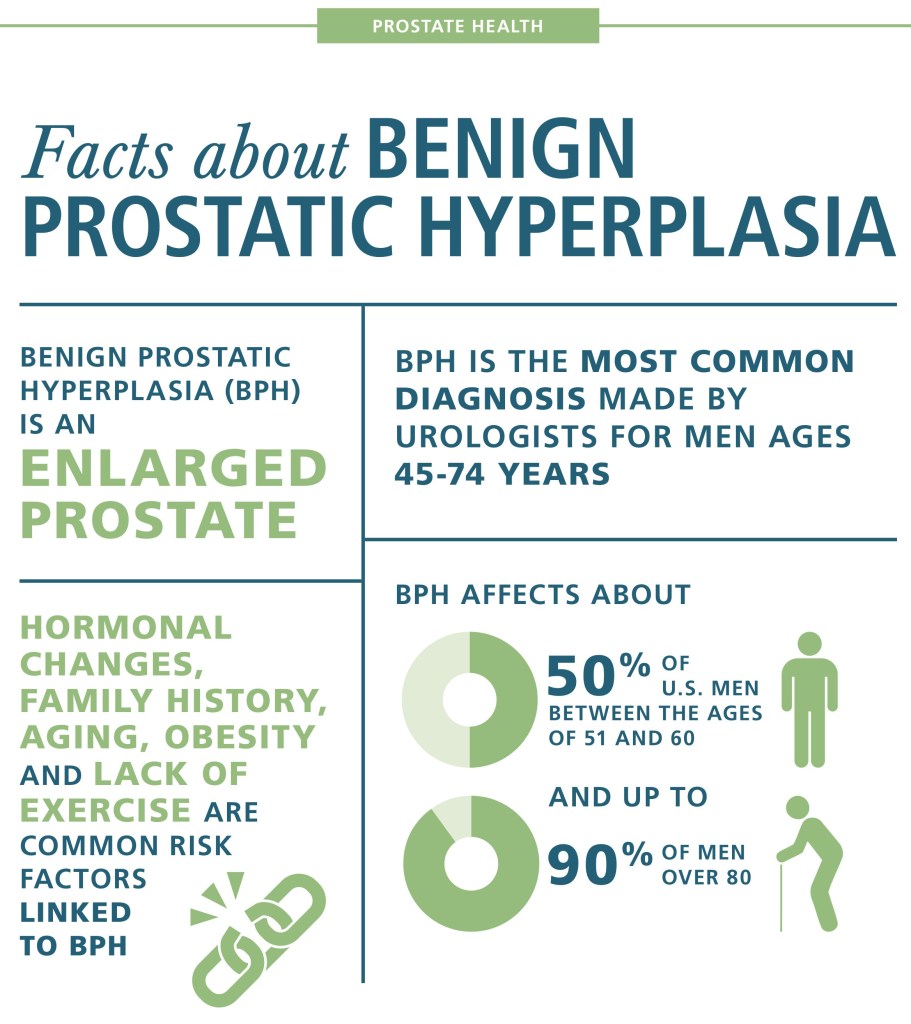
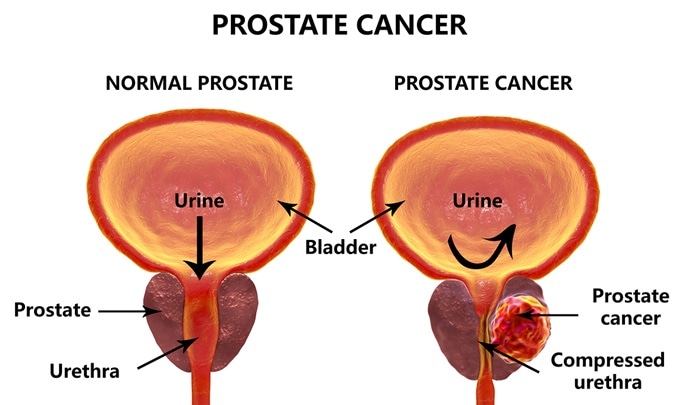
I have known about the Prostate gland, which surrounds the urethral channel exiting the bladder, since med school. I have seen evidence of its enlargement in the increasing time it takes older men to empty their bladders.
When my dad had his prostate surgery, he said that he could blast the porcelain right off the toilet, I could then appreciate for the first time that enlargement of the prostate caused a weak urinary stream.
When I started waking up at night 3 or 4 times to urinate, it really hit home. I had to get something done. My Urologist was a very good one, like all of my doctors. As the old saying goes, the best is none too good when it comes to your health.
On my first visit, he ordered a “Urodynamic” study. In this test, done by a visiting nurse who had the equipment, a small catheter, or tube, ws passed into my bladder, after loading myself with water until I could hold it no longer. The pressure in my bladder was measured, the speed with which I evacuated my bladder was measured, the volume of urine I passed was measured, as well as the volume retained in the bladder.
With these numbers, my bladder volume, residual, and the resistance to flow was calculated. I was shown to have a small bladder, too much residual retained after I emptied it, and an excessive resistance to the flow of urine out of the bladder.
I have not seen the urodynamic studies mentioned in the modern workup of BPH, and it may not have been critically necessary. I did appreciate his thoroughness, however, and factored in the study when he gave me the options of medicine vs. surgery.
were two medicines mentioned, an alpha adrenergic agonist, and finasteride, an anti-androgen. Since I would have to take both meds the rest of my life, I chose surgical enlargement of the urinary passage through the prostate, known technically as a “roto rooter job”. I, too, noticed the power of my urinary stream after the surgery.
A good friend of mine, also a physician, took medicines for many years, in spite of increasing trouble urinating, getting up at night, and frequent bathroom trips during the day. He eventually went to see a urologist after he had to go to the ER for completely being unable to pass urine.
The Urologist declined to do surgery on the basis of his health, the unusually large size of the blockage, and degree of obstruction. He used a catheter to relieve himself several times a day for the rest of his life. Had I been in his shoes, I would have tried to find a willing surgeon somewhere, perhaps at a university med school.
But then again, I wouldn’t have waited so long. These days many more options are available, and the appended article discusses some of them. –
Prostate cancer is perhaps the most common cancer in men. It increases in incidence with age, and if you live long enough, most men will contract prostate cancer. A family history of cancer and obesity are also risk factors. But many times the cancer is so slow growing that it will not kill you. In the age of modern, aggressive medicine, the treatment has often been worse than the disease.
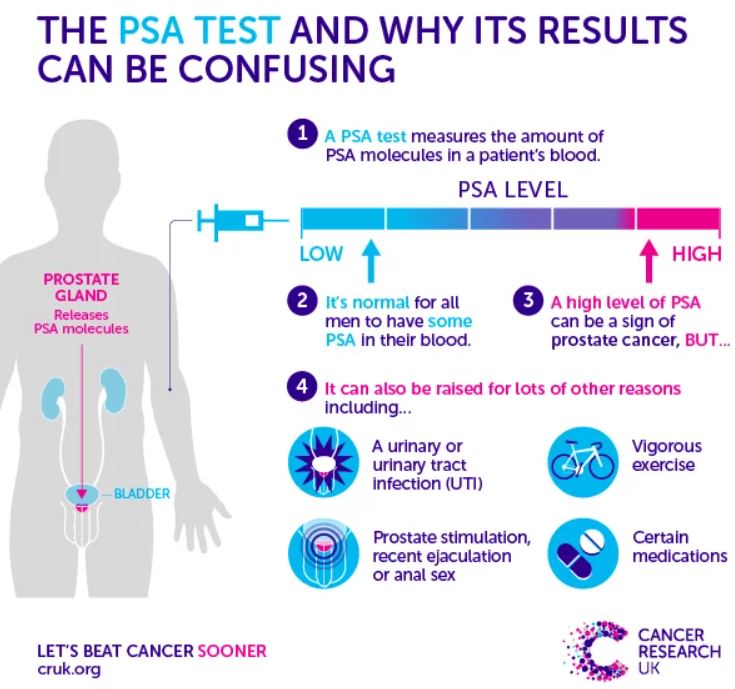
Treating Cancer EARLY is much more successful. The PSA test was one of the first really sensitive blood tests for cancer, and it was once performed routinely, on a yearly basis, usually at the time of your annual physical.
The PSA (Prostate-Specific Antigen) test is VERY sensitive,however. In responding to an elevated PSA, very slow growing tumors would often be treated aggressively, creating more morbidity than the untreated tumor would have caused.
The treatment seemed to be worse than the disease. Many physicians stopped doing the PSA test altogether, relying on symptoms, or detecting an abnormality on RECTAL EXAM to trigger an investigation. Some years ago, a physician friend of mine elected to stop PSA testing, and two years later was discovered to have METASTATIC Prostate cancer. It had already spread to his bones, and he eventually died of that cancer.
This encouraged me to continue with PSA screening, though it is still considered optional. Very recently, a test has been developed which I think tips the scales back toward annual PSA testing. EXOSOMES are little (10-120 nm.) particles that effuse from many cells, especially cancer cells.
They contain a variety of DNA, RNA, proteins and lipids which allow the cells to communicate with one another. Recently, a company, ExoDx, was created to take commercial advantage of Exosomes in the diagnosis of various diseases, by testing body fluids.
Their test, ExoRx Prostate EPI test of urine, has been shown to be helpful in distinguishing AGGRESSIVE prostate cancer from the slower growing kind, when the PSA test is in the “grey zone” between 2 and 10 ng/ml. PSA test results above 10 ng. were always acted on, especially if the numbers were increasing. I would be surprised if the PSA did not reenter the annual testing protocol.
The annual digital rectal exam in men older than 50 years will continue to be done, although it is not very sensitive, and is often not abnormal until the cancer is more advanced. Pain in the prostate area, blood in the urine or semen, and trouble urinating are symptoms worth investigating, but if cancer is detected, it may well be advanced and harder to treat. With abnormal tests,
Risk factors or suspicious symptoms, further testing is often done. Ultrasound or biopsy may be indicated. Sometimes the biopsy is guided by MRI, to increase the likelihood that the cancer, if small, is included in the tissue sample taken. Examining the cells of the biopsy sample will yield a “gleason score” which grades the aggressiveness of the cancer.
This in turn dictates the treatment, which may include different extents of surgical removal, radiation, hormonal or chemotherapy treatment. None of this is pleasant, and you are better off, of course with prevention.
Our old friends, DIET AND EXERCISE are thought to be helpful. Although not proven, eating lots of fruits and vegetables, and maintaining a healthy weight are recommended.
–DR. C
Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.
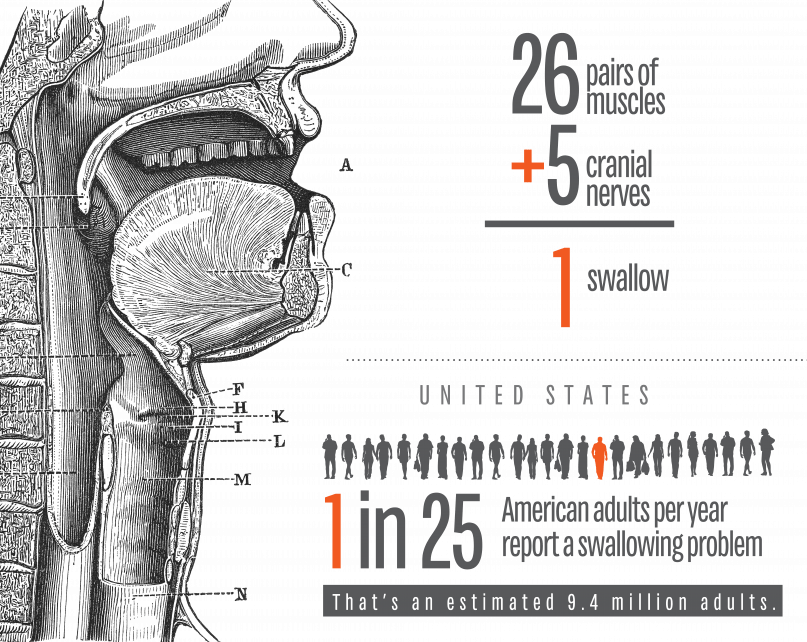
I am defining SWALLOWING TROUBLE as the difficulty in transport of food to the stomach, once clear of the throat. Problems with the initiation of the swallowing process are discussed separately.
PAIN in the mid-chest ON SWALLOWING is a worrisome symptom which can be due to inflammation of the lining of the esophagus from a variety of causes. An esophageal yeast infection, which can also involve the throat (called ‘“thrush”), often warns of immune deficiency and can be a sign of AIDS, or be caused by immune suppressing medication. If persistent, pain on swallowing can be a warning sign of CANCER.
If in the presence of GERD, it can be a sign of chronic inflammation or ulceration. In-coordination of the normally smooth muscular propulsive wave can cause a cramping, muscular pain.
Normal “peristalsis” is so efficient, that food can be swallowed without the help of gravity, when UPSIDE DOWN. I wouldn’t recommend trying this, even to cure hiccoughs. There is a muscular “gate” at the bottom of the esophagus, just as it enters the stomach. This gate is often too relaxed, and allows for the reflux of acid and food from the stomach, or GERD. It can also Fail to open, called achalasia, and hold up the food in its journey to the stomach.
The area can be scarred by repeated acid reflux, and become NARROWED; this is called a STRICTURE, and can cause a blockage in swallowing. One of my Doctor friends had to go to the Emergency room when some Steak got stuck in the esophagus.
The ER Doctor removed the steak with a fiberoptic Scope, and then proceeded to DILATE the stricture with a “bougie”, an instrument of a precisely calibrated size designed to STRETCH the constricted area. This uncomfortable procedure had to be done repeatedly, a caution to those who would wait too long before getting such a problem evaluated and corrected.
EOSINOPHILIC ESOPHAGITIS has been diagnosed with increasing frequency, and can cause Pain in the middle of the chest, trouble swallowing, and even regurgitation of food. This special type of inflammation is more common in allergic patients, and can be caused by certain foods.
So as you can see, swallowing trouble, if persistent, is nothing to fool around with, and should be checked out by a competent doctor. Don’t wait too long.
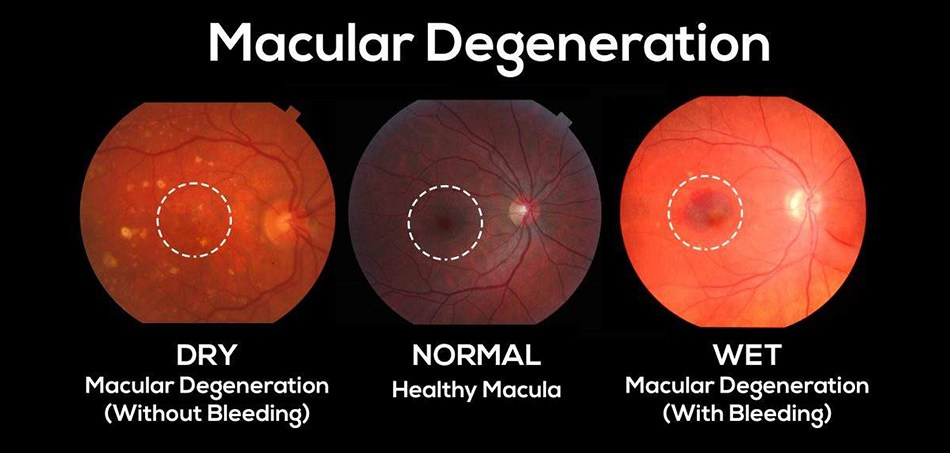
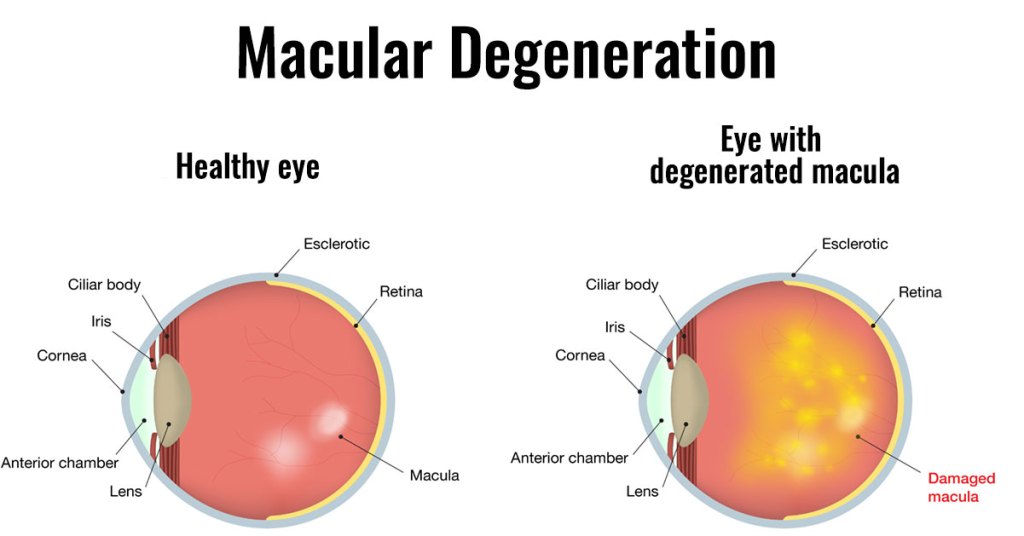
Macular Degeneration is the most common cause of blindness in the western world.as you get older, it becomes increasingly common, and almost 20% of people older than 85 years have this disease.
It comes in 2 types, dry and wet. Mostly it starts as the milder dry type, which develops slowly and has no definite treatment. The dry type can develop into the more rapidly progressive wet variety, however, and is important to notice and report to your ophthalmologist.
The MACULA is the center of the visual field, and has by far the most photoreceptors. It yields the sharpest vision, and is essential for reading, and even recognizing faces.
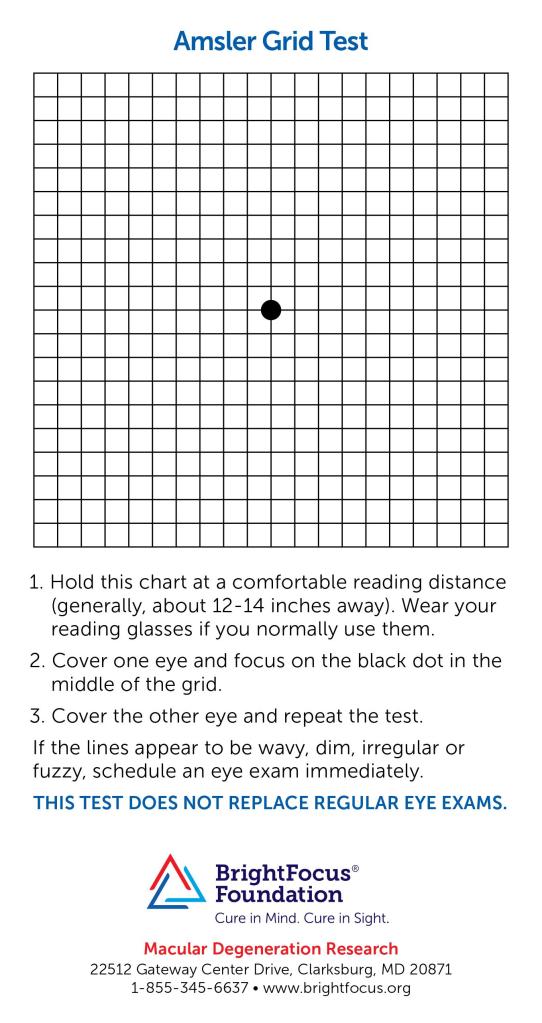
LOSS OF VISION is the commonest symptom, but is hard to notice in a slowly developing condition. A neurologist friend of mine alerted me to the AMSLER GRID, which helps in picking up the subtle distortions of this sneaky problem.
Checking your vision every few days-it takes only a few seconds- is a good idea as you age. You might be healthy in every other way, but if you are blind, the quality of life in your final years will suffer. The mechanics of the wavy lines generated by macular degeneration are deposits beneath the macula, raising it up.
The deposits are fatty in the case of the dry, and fluid in the case of the wet macular degeneration; and fluid from the abnormal blood vessels in the wet MD can collect very rapidly indeed.
Even though the cause of MD is unknown, prevention is by the same old healthy habits tiresomely mentioned in all my other postings: DIET and EXERCISE. I’m sure that good sleep doesn’t hurt either, No cigarette smoking of course, and there are some vitamins and minerals mentioned, such as lutein, zeaxanthin, zinc, and copper.
The wet MD does have a treatment to slow down the disease. Since blood vessel growth is important in causation, antibodies to VEGF, vascular endothelial growth factor, are injected into the macular area. I’m sure that more help is on the way. Some treatments to support the protective pigmented layer of the retina are currently in progress.
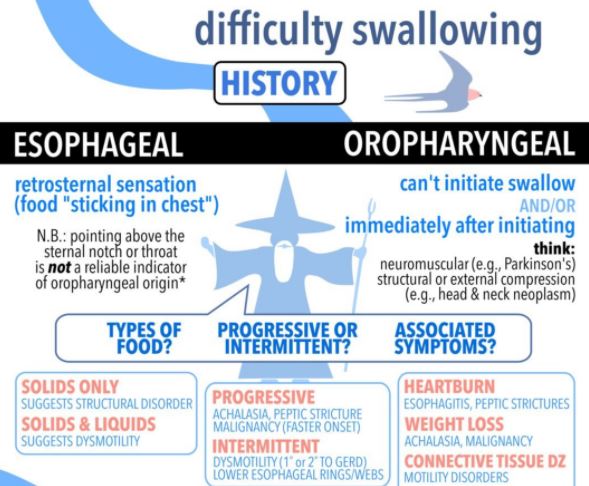
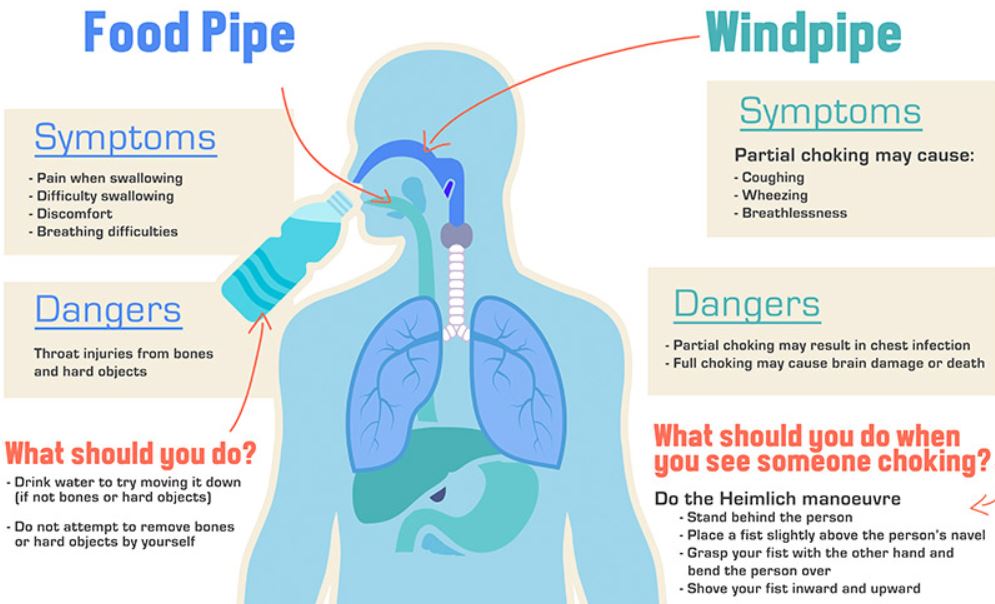
DYSPHAGIA covers a wide range of troubles, symptoms and diseases, as indicated from the excellent Infographic posted August 21, 2020. I have already discussed GERD, or trouble with the food coming back up after being swallowed.
This post will be on “choking”, or getting the food into the Airway instead of the Esophagus, or swallowing tube. In the future, I will develop a post in “swallowing difficulties”, or trouble getting the food to pass easily and freely down the esophagus into the stomach.
CHEWING the food properly is rare in our rushed, fast-food society, but it is very important, the first part of the digestion process. Mastication breaks the food into smaller particles that are easier to digest, and also EASIER TO SWALLOW. Saliva flows as you chew, and contains Ptyalin, an enzyme which breaks down starch into absorbable sugars.
Chewing also SLOWS down the rate of eating, improves enjoyment, and allows more time for the stomach to send Satiety signals to the brain. This leads to less overeating and weight gain. In children, chewing is said to aid in jaw development and to reduce dental crowding and need for Orthodontia.
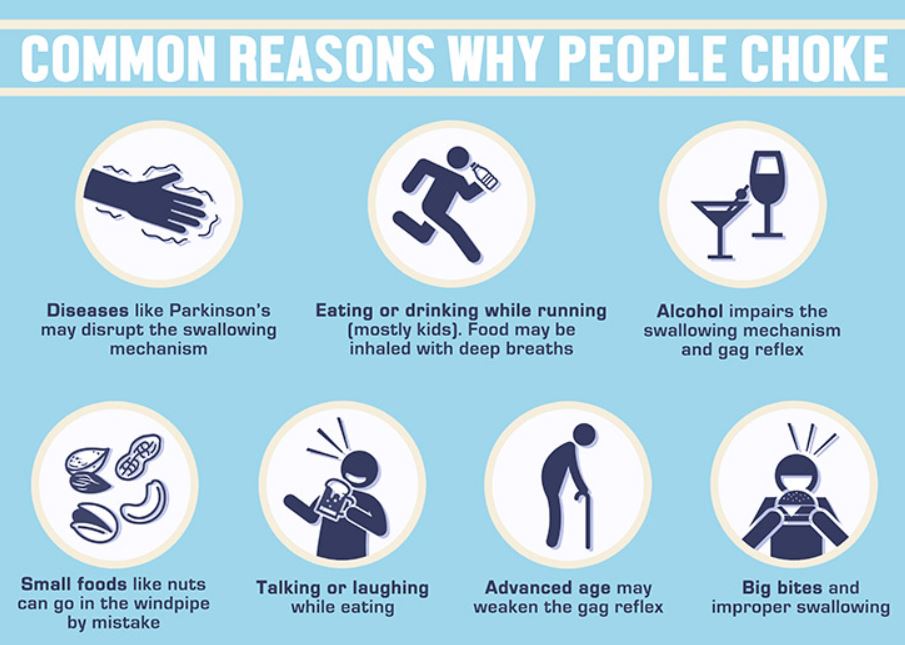
Some people have trouble in Initiating the swallowing process. This can be caused by neurological problems like Parkinson’s Disease. It can also be Psychological, a reflection of fear of discomfort on swallowing.
I have the opposite problem, a tendency to swallow too eagerly and rapidly, causing me to choke on liquids, sometimes even on water. I went to an ENT specializing in swallowing problems. He checked the sensitivity of my throat to touch, and found it normal.
Apparently LESSENED sensitivity is the main concern, which would lead to Aspiration of food. The only guidance he gave me was to eat and drink more slowly. I find that I am most likely to choke when I drink wine, or a tasty beverage which I tend to “slurp” so as to fan the aroma out broadly in my mouth. I am having a hard time breaking myself of that habit.
Sometimes I find that residual amounts of food builds up in the back of my throat, probably by my epiglottis. I worry about nuts especially. If I don’t drink some water to flush it away, I am likely to choke on it. I guess that is the reason people are told to offer some water to a person who is choking.
I seem to be choking more as I get older, which is reasonable. Swallowing requires an amazingly intricate coordination and motion in the throat area, especially in getting the epiglottis, the little door that closes off the windpipe, to close properly.
My other dexterities are fading, why should swallowing be an exception? Pill swallowing is getting more frequent and more problematic at the same time.
Tablets are worse than capsules, maybe because they are not as slick. There is one size in particular that tends to get stuck in the back of my throat just above the uvula. I sometimes have to cough a lot and choke the offending object back up. One more reason to constantly try to cut down the number of pills.
There is one good thing about this problem, however. I now take the pills separately with a big swallow of water, improving my Hydration.
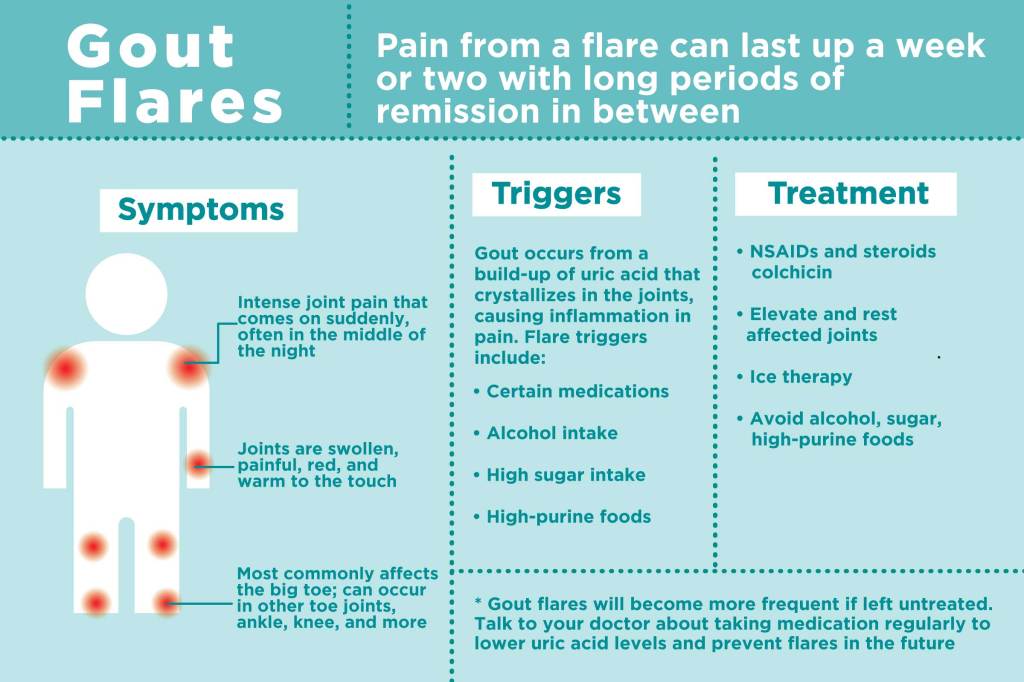
If you develop severe big toe pain in the middle of the night, and it is so tender that you can’t even stand the pressure of the sheet on it, you may have GOUT, an increasingly common form of ARTHRITIS.
And you would be in famous company: King Henry Vlll, Isaac Newton, and Benjamin Franklin all had Gout. There is even a famous dialogue between Franklin and his Tormentor.
Gout is caused by a buildup of URIC ACID in the bloodstream. This buildup can be caused by eating too much nucleic-acid-containing foods, like meats, “sweetbreads” and shellfish, and drinking too much alcohol, especially beer.
Reduced Clearance of Uric acid in the kidneys may contribute, and may be responsible for some of the familial tendencies of gout. The uric excess acid in the blood stream gets into joint tissues, most famously the big toe, although ankles, knees and other joints may be involved.
When deposited in joint tissues, the uric acid crystals attract inflammatory cells, which secrete their Interleukins and produce all of the symptoms of painful, red and swollen joints.
Risk factors include Obesity, diabetes, and the usual suite of problems of the METABOLIC SYNDROME. Just look at a picture of Henry Vlll with a mug of beer in one hand, and a leg of mutton in the other, and your big toe will start to hurt.
Dietary regulation is one of the best ways of reducing PURINE AND PYRIMIDINE intake and consequently the metabolic BYPRODUCT, Uric Acid, in the circulation.
There are DRUGS, called uricosurics, which will cause the kidneys to Clear more Uric acid, and other drugs, such as thiazide diuretics, which will reduce clearance and excretion of gout’s causative agent.
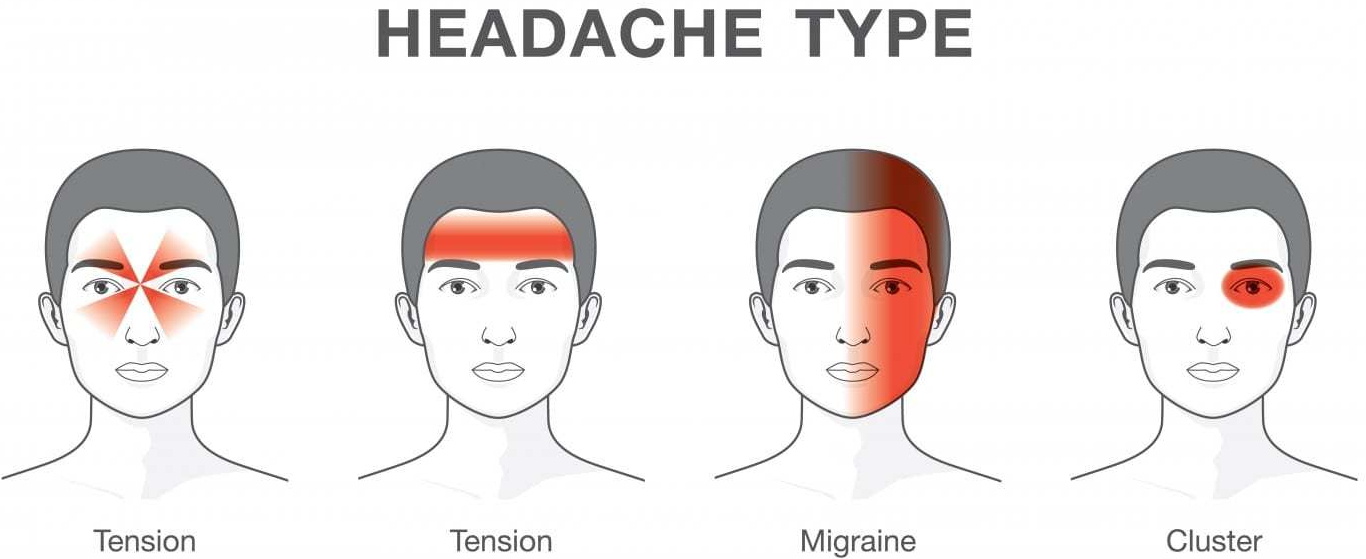
Headache has been with us since Neolithic times, and has caused enough distress to induce our ancestors to scrape holes in their skulls, perhaps to let out the causative Evil Spirits, or maybe a subdural hematoma.
When I was a practicing Allergist, i was sent many headache patients by other Doctors.This was, presumably, because the referring physician thought that their patients had “sinus” headaches. In fact, free standing headache does not commonly come from the sinuses.
Most headaches thought due to ‘sinuses” are in fact “vascular “ headaches. The theory of vascular headaches is that the average diet contains many chemicals that are active on blood vessels. Tyramine, degraded proteins and caffeine are examples. These chemicals, working on the blood vessels, cause irritation and pain. It follows,then, that avoidance of these chemicals would relieve the vascular headaches.
“Vascular headache”, and it’s severe cousin, Migraine headache, is now included under PRIMARY HEADACHE, which also includes Tension headache, and a variety of less common diagnoses. But it is still useful for Treatment, which is why I use the term.
My treatment was a fresh, “health food” diet which avoided preserved foods such as salami, sausages, sauerkraut, leftovers, cheeses, red wine and a variety of other foods likely to have degraded amino acids and Tyramine.
The “mold-free diet” was the published diet closest to listing the suspected foods. The benefit reported from the diet encouraged me to continue recommending it. Vascular headaches are essentially a mild variety of migraine headaches. The foods avoided in the “mold-free diet” are still, after several decades of progress still recognized as migraine triggers.
I encountered only one patient with BRAIN TUMOR in my practice. She had severe, unremitting, gradually increasing headaches over a 4 week period. I called a Neurologist, the type of doctor that treats most severe headaches, who informed me he had NEVER seen a patient with a brain tumor who presented with a headache only, so uncommon it is.
Tension Headaches are milder, and usually can be handled at home. These headaches are usually accompanied by tenderness in the muscles of the back of the neck, or in the temple region, and are brought on by stress.
Hypertension, if extremely high, can cause headache, and can be dangerous, but I never saw a case. Nor did I attend a patient with temporal arteritis, which can also be an emergency.
There are some “red flags” that indicate urgent need for evaluation:
New headache in older patient
New change in headache pattern, or progressively worsening headache
Signs and symptoms of illness ( fever, stiff neck, rash).
Headache triggered by cough or exertion.
Headache in pregnancy or postpartum period
First, worst Headache.
New headaches with AIDS, compromised immunity, or cancer.
Headaches accompanied by mental changes, weakness, or abnormal Neurological signs.
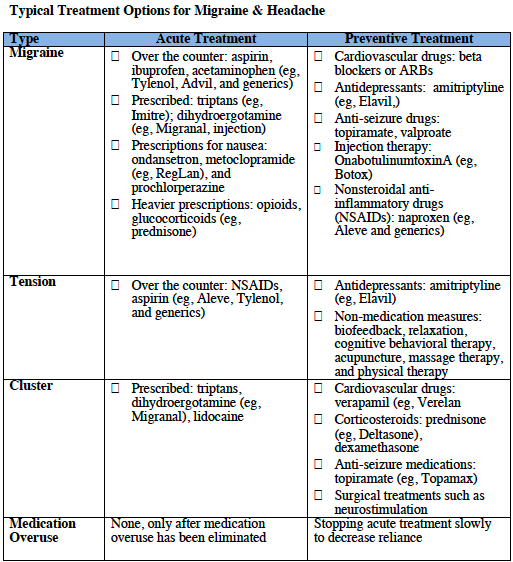
Selective medications are available for some headaches.
Preventative and abortive medications sometimes are helpful for migraine. Antidepressants, tryptans, beta blockers, and corticosteroids are medications best prescribed by specialists.
The tendency to use pain killers, especially narcotics, must be tempered. Frequent use can create additional problems, like ADDICTION. The CAUSE of the headache must be found, if possible, and specifically treated.
Of course, I did find patients with true SINUS HEADACHE, but the headache was accompanied by fever, tenderness over the sinuses, yellow nasal discharge, and other evidence of SINUSITIS, and went away when the infection was treated.
If you have a lot of headaches, and no “red flags” or “risk factors”, you might try a “mold free diet” for a few weeks. Your Nutrition and health would certainly not suffer. And you might have fewer headaches!
Please read the following article for a more complete discussion of this common and annoying problem.
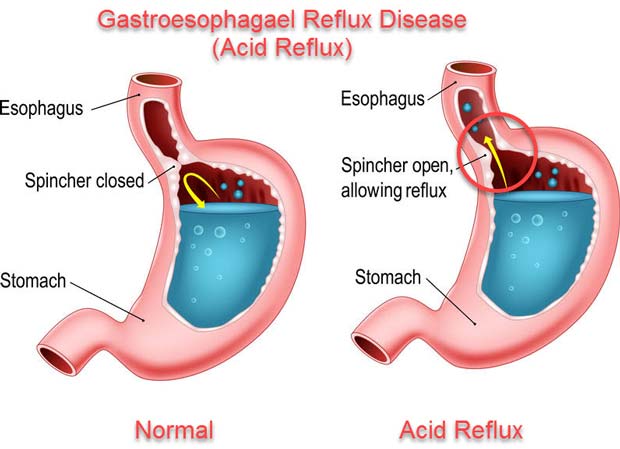
I have been having Heartburn for more than 40 years. The cause of Heartburn is leakage of acid from the stomach, where tissues have evolved to tolerate the highly acidic conditions, into the esophagus, where they haven’t.
The young body has an efficient, functional gate, or sphincter, keeping the food, once swallowed into the stomach, from coming back up. As you eat, you chew your food well to aid digestion. Your taste buds, sensing chemicals in the delicious food, activate saliva.
The salivary enzymes start the digestion of the carbohydrates in the food. If you eat slowly enough, you may be able to appreciate the digestion of tasteless starch, like in bread, into sweet sugar, right in your mouth.
You then swallow the food, which slips past another gate, called the epiglottis, diverting the bolus of food past your windpipe. This gate sometimes does not shut tight, and you choke on the food or drink. The food is then conducted into the highly acidic environment of the stomach.
The stomach evolved to be an acidic, “fiery pit”, inhospitable to any bacteria that came in with the food, thus protecting the stomach from infection. In the old days, there were a lot of bacteria, and the acidity of the stomach was useful, and evolutionarily conserved.
These days, the “fiery pit” tends to be a problem. As you get older, the gate that keeps food in the stomach gets more floppy and relaxed, and allows food to come back up into the esophagus, and sometimes, most often at night when you would rather be sleeping, all the way up to your throat, and is inhaled into your windpipe and lungs in what is called “gastroesophageal reflux”, or GERD.
Even if the food, and acid, doesn’t make it all the way up, and stops at the esophagus, which has not evolved to tolerate acid, you will have “heart burn”. Of course it is not the heart that is burning, but the esophagus, which runs right past the back of the heart as it goes all the way from the throat to the stomach.
When I first developed Heartburn, all that was available was the flavored chalk, Calcium Carbonate, sold as Tums. It works right away, and is a source of Calcium, but can cause trouble, like kidney stones, if you take too much. The relief didn’t last long enough for me, and I had to take more in the middle of the night.
My next medicine was Xantac, a medication that blocks histamine from stimulating acid production in the stomach. The H2 blockers have recently been recalled because of NDMA contamination. I sometimes used H2 blockers like Xantac when my patients would get a bad allergic reaction. In such cases BOTH an H1 blocker like Benadryl, and an H2 blocker are called for.
Zantac was not strong enough for me, and I soon graduated to Prilosec,which directly blocks the secretion of acid in the stomach.
Prilosec was then very expensive, but now is available as the inexpensive GENERIC Medication, Omeprazole. It seems that no medication is without side effects.
Omeprazole, by reducing stomach acid, makes stomach and GI infections more likely, and interferes with the absorption of B12, and Calcium.
If you have had a lot of heartburn over a long period of time, you should check with a Gastroenterologist, who may scope you to rule out Barritt’s esophagus, which can lead to Cancer.
It is interesting that the antacid Tums in excess can cause too MUCH Calcium in the body, and can cause kidney stones and other kidney problems like MAS, and Omeprazole, by interfering with absorption can cause too LITTLE absorption of Calcium, leading to OSTEOPOROSIS.
The best rule is to take as low a dose of ANY medication as possible, preferably none, to understand the possible side effects, and compensate for them if you can.
As I have aged, my skin has been more itchy. My allergy practice was loaded with Patients whose ECZEMA and HIVES itched. My favorite uncle developed intolerable itching (pruritis) in his 90’s, and died within a year of metastatic Prostate Cancer.
This gives you an idea of the Range of this annoying sensation. My emphasis here will be on CHRONIC ITCHING with DRY SKIN in otherwise HEALTHY PEOPLE without much rash or other skin condition. If you want extra discussion, look at Reference #1. If you are a Doctor, or a brute for punishment, see Ref.#2, a CME review.
Your skin is the largest organ in your body, and deserves respect right from birth. The skin of your child is wonderfly healthy in looks and self repair. EXCESSIVE SUN EXPOSURE is about the only thing you need to protect her from, and the only penalty is increased cancer risk in later life.
As your body ages, your skin looses some of its essential oils, and and becomes more dry (at least you don’t get acne any more). You become more sensitive to dry air, like in the winter, when the cold outside air (adiabatically) drops in relative humidity when warmed to inside temperature.
Do you notice the increase in static electricity shocks in the winter? If not, I’m sure that you do notice that your skin itches more. one treatment for the “winter itch” is to humidify the inside air. If you have a draughty old house like I do, it may be more convenient to use MOISTURIZING LOTIONS.
These were once mainstays of itch control in my former practice (before development of the effective modern medications). Eucerin and Cetaphil were very helpful. Maybe it is because of the name, but I now find myself using Curel “Itch Defense” all over my body twice daily,.
The itching is much less now, except for my EARS. My ear canals (they are skin too!) have recently been very dry and itchy, maybe because i listen to podcasts when walking or swimming.
Unwilling to give up my podcasts, I put some UNSCENTED Johnson’s baby oil with my little finger into my ear canals, as suggested by my ENT Doctor (I wanted to be sure i didn’t have a diagnosable condition like a fungal infection). If I have a small spot that itches a lot, I use some 1% Hydrocortisone cream, and I feel better.
Antihistamines don’t do much for me, but are effective if the itching is a real allergy (most of what people call allergy is not the IGE-MEDIATED, “real” variety). HISTAMINE is the quintessential provocateur of ITCH. Cetirizine (or atarax) is the strongest of available antihistamines, and diphenhydramine (benadryl) the old standby.
Chronic itching can be caused by a plethora of illnesses, as you will find if you choose to read the following papers.


 Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.
Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.