

The goal of #ACL surgery is to rebuild or reconstruct the ligament. It allows many athletes- like basketball players- to get back on their feet after an injury.
— Mayo Clinic Sports Medicine (@mayoclinicsport) March 31, 2022
Learn about the surgical and non-surgical options our ACL Specialty Clinic has to offer. pic.twitter.com/OAU0QjemkF
Tag Archives: Knees

DR. C’S JOURNAL: PAIN FOLLOWING TOTAL KNEE REPLACEMENT SURGERY
Total knee replacement(arthroplasty) is one of the most successful orthopedic operations. Satisfaction rate varies between 75 and 90%. Even so, almost 10% of operated individuals will have anterior knee pain, the most common complication, 1 year after TKR.
I had an even greater appreciation of the knee after reading the following article, which explain the causes of knee pain more adequately than I can, and would be good to read.
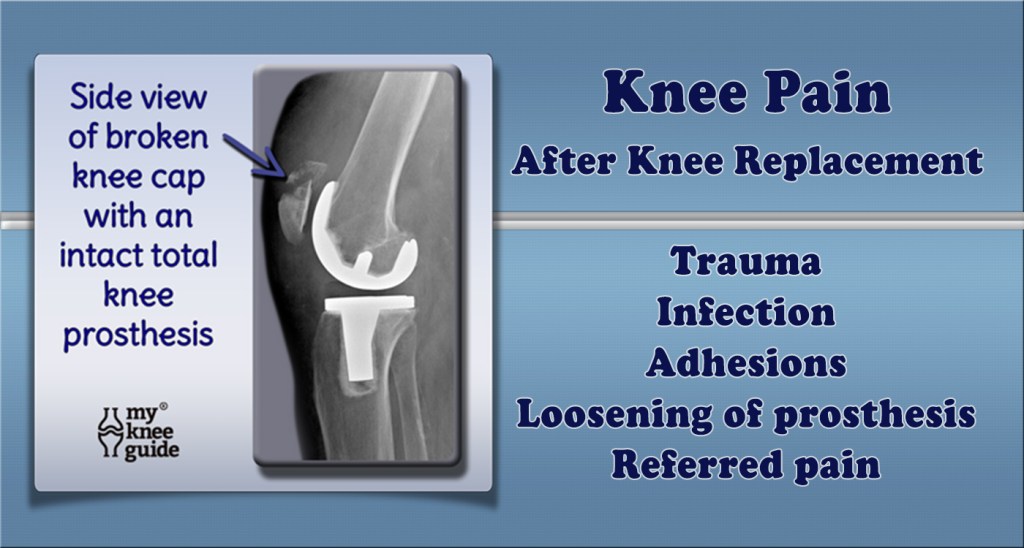
With knee replacement surgery, a great deal depends on the technical expertise and precision of the operating surgeon. A rotational error more than a degree or two can be critical, so important is proper tracking of the kneecap in the trochlea, or groove in the leg bone(femur). An imbalance in the pull of muscles, or a knock knee, (Valgus) angulation of the knee, hip rotation, spinal problems, all can be important in generating pain as you get older.
There are psychological factors too. The knee pain after TKR average is only 1/3 of that suffered before the operation, on average. However if you expect that discomfort will disappear completely, or if your pain threshold is low, or if you have anxiety or depression, you may have more postoperative pain, and be disappointed with the surgery.
My immediate reason to write this article was the anterior knee pain developing in a friend of mine, 15 years after surgery, at the age of 89. She had polio in childhood, and her right leg was severely affected. This caused her to overuse her left leg, resulting in a TKR 15 years ago. Just recently, she started developing anterior knee pain in the left knee. A thallium scan showed a lot of signal on the inside of the kneecap, most likely indicative of inflammation. She is not enthused about having another operation because of her age., and wondered about other things she might do.
An orthopedic friend of mine suggested that injections of a viscous lubricant might help, if the initial operation did not include resurfacing of the kneecap (patella). I would imagine that eventually the resurfacing of the patella with advanced materials, or perhaps stem cells might help.
I also thought of a special brace with a motor assist for her right leg, but the orthopedist said that this did not work very well in polio patients, who have a weak nerve signal.
Although my friends polio made her TKR almost inevitable, there are things that you can do, or avoid doing, that could help avoid TKR. Activities to reduce include squatting, deep lunging, running (particularly in deep sand), high impact sports, repetitive jumping, and running up stairs. Basketball, football, and volleyball come to mind as regular sports that are risky. Maintaining a healthy weight, controlling blood sugar, stoppage of smoking, avoidance of injury, and regular exercise, particularly walking and swimming ,are things that might help.
Remember that your knees are your wheels and are jewels to protect as you get older.
–Dr. C

Mayo Clinic: ACL Tears – When Surgery Is Needed
ACL tears can sideline an athlete or crush an Olympic dream. It’s a common knee injury affecting nearly twice as many women than men. Dr. Cedric Ortiguera, a Mayo Clinic orthopedic surgeon and sports medicine specialist, says 150,000‒200,000 ACL injuries occur each year in the U.S., and that number is growing as more children become involved in competitive sports year-round. The good news is that surgery can help get some athletes get back in the game.

THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #6: OSTEOARTHRITIS (OA)
Osteoarthritis (OA) was considered a Degenerative disease when I went to Med School in the late 50s. I am more interested in OA since I have developed it myself.
There is a 40-60% hereditary component. My father’s mother had arthritis badly in her hands, as did my mother’s mother, and so on. A lot of genome-correlation work has shown many different genes involved,
But without a single big contributor, OA appears to be “multifactorial”, similar to a lot of common diseases like Diabetes l. Trauma can be a factor. Old sports injuries, like an ACL tear, that you thought a thing of the past, may come back to haunt you in later years.
INFLAMMATION, the most popular explanatory cause of the decade, may be operating in OA. For instance, you can imagine that OBESITY would contribute to hip and knee OA simply through the traumatic force of gravity. But obesity is also a disease of Inflammation, and increases IL-6 and other cytokines as well.
My own OA involves the classic distal 2 interphalangeal joints (go to the wikipedia manekin for a color-representation of OA classic locations). The base of my thumb, neck and back are also a problem.
Strangely, but wonderfully, my “wheels”, the Hips and Knees, are spared. I have exercised a lot in my life. Clearly, you can’t “wear out” your joints with ordinary exercise.
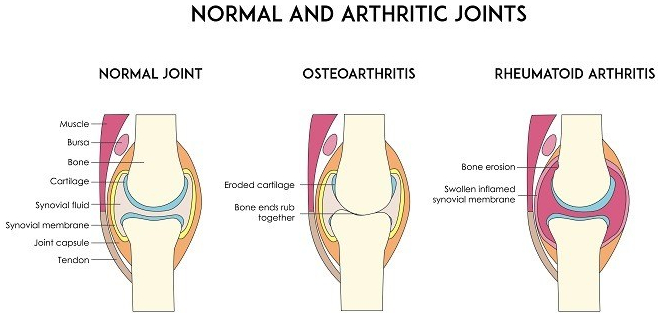
Our joints have evolved to allow us to move. Since bone has a lot of pain fibres, it would be painful to move the joints, directly bone-on-bone. So we have cartilage on the ends of the bones and discs between the vertebrae. The cartilage is slick to reduce friction.
Cartilage has no blood to supply it with nutrients. Instead, it relies on the joint (synovial) fluid. The cartilage is like a sponge. Walking alternately compresses and relaxes the spongy cartilage, increasing the synovial fluid circulation, thus improving the nutrition of the cartilage. If the Cartilage disappears, there is pain.
I am not a fan of pain medication. My belief was strengthened by the side effects of the study of a medication designed to genetically block pain transmission by injection into the painful joints. The side effect was virtual dissolution of the joints in a fraction of those treated. I felt more comfortable with my pain after reading the article.
Although Acetaminophen helps a little, NSAIDs usually work better, perhaps because of their anti-inflammatory action.
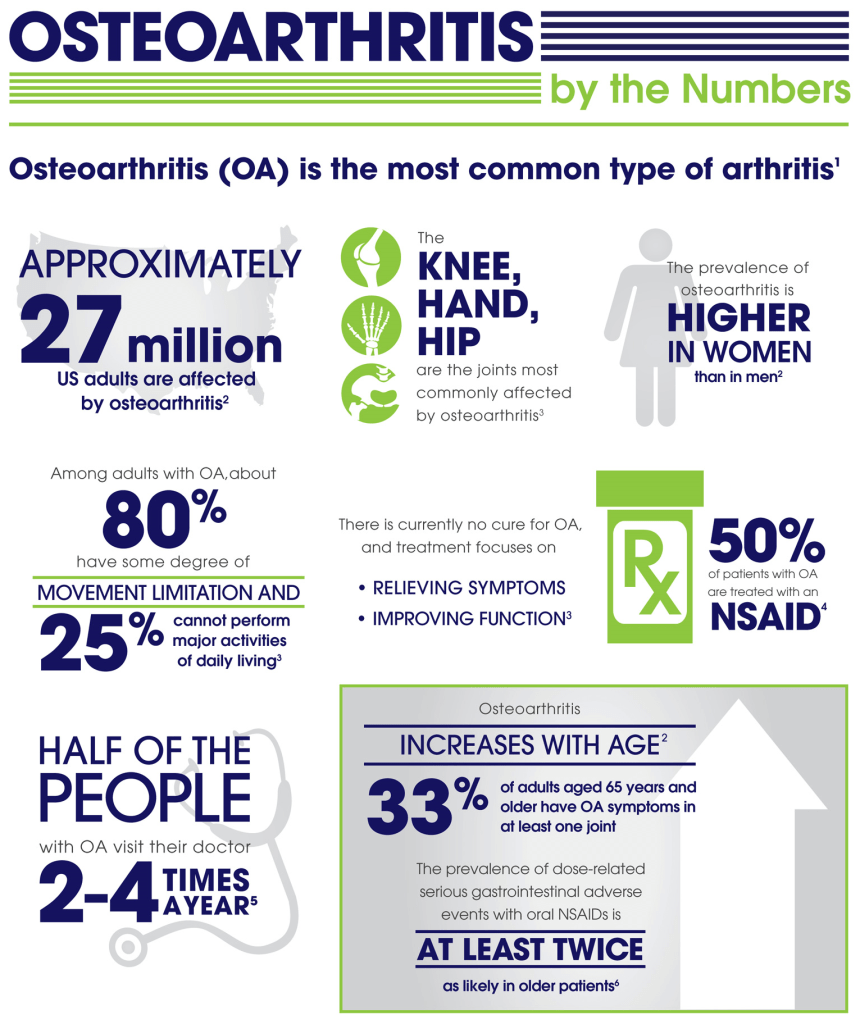
If, like me, you have stomach issues, there are the COX-2 inhibitors like Celebrex. The one dose I recently took was almost magical in its effects. Maybe if you don’t use pain Meds much, they work better.
I do take Glucosamine-Chondroitin, thinking that providing building blocks for cartilage couldn’t hurt. Along this line I also EAT CARTILAGE whenever I eat Chicken or ribs, being careful not to damage my teeth in the act of of exercising my jaws.
I also take Curcumin, hoping to relieve some pain, in spite of the fact that it is poorly absorbed (some brave souls take it by injection). I don’t know if any of this helps, How can you know in such a variable disorder, in the absence of controlled studies.
And pain has no OBJECTIVE markers, and is notoriously hard to study. We literally know more about the surface of mars than we know about Pain.
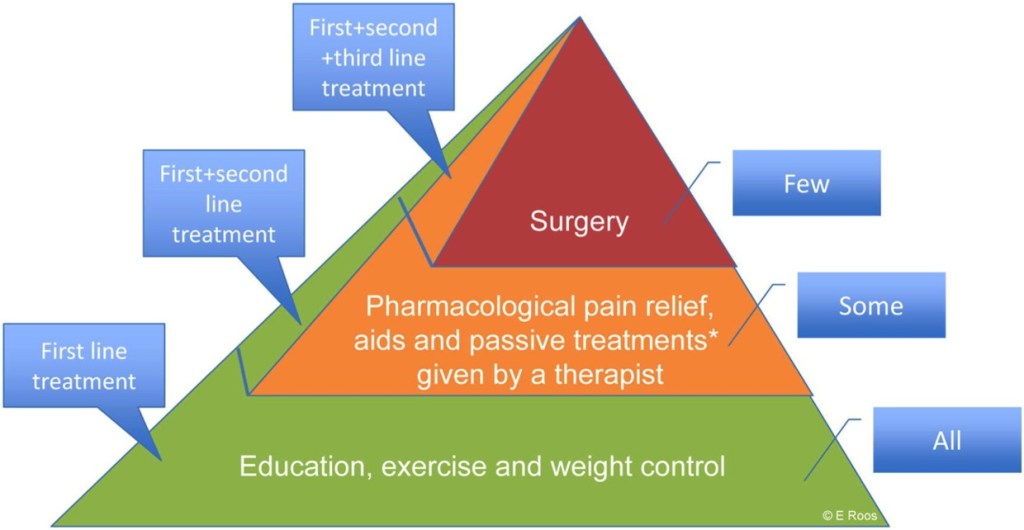
SLEEP, DIET, and EXERCISE, by minimizing OA factors kike OBESITY and INFLAMMATION are the best bet for preventing and treating OA at present.
