

BLOOD VESSELS; it is hard to overestimate their importance. They are literally our lifelines, delivering the oxygen and nutrition necessary for life. We are as old as our blood vessels.
I will divide blood vessels into 4 components with rather separate domains: The Systemic Arterial system, the Pulmonary circulation, the Venous system, and the Lymphatic system, and will discuss these separately.
SYSTEMIC ARTERIAL SYSTEM
The Boy Scouts taught me the pressure points; The radial, at the thumb-side of the wrist, the brachial, on the inside of the upper arm, and the inguinal in the groin area. Pressure on these sites will stop arterial bleeding distally.
You should be able to locate the radial artery pulse, and begin to appreciate its strength and regularity. Strength in case you encounter a person who isn’t moving, and regularity for yourself; many older people develop an irregularity called Atrial Fibrillation, and you might be the first to discover it..
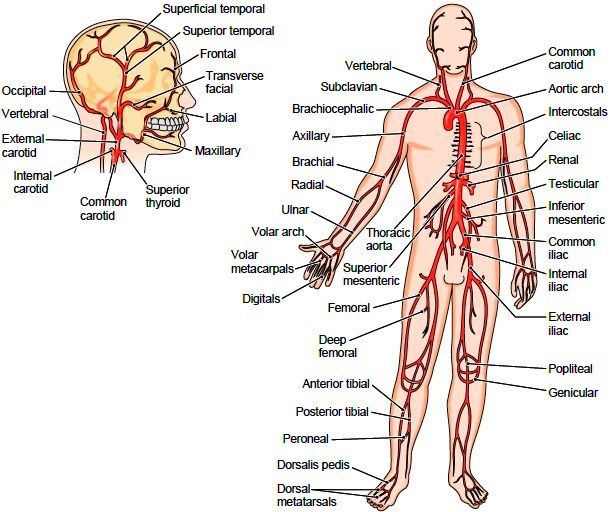
ANEURISMS are swelling of the arteries, and the swelling may thin the arterial wall so that it can burst. A Cerebral aneurysm can burst and cause a stroke-like problem. If an aortic aneurism bursts, the internal blood loss can be fatal.
RAYNAUD’S Phenomenon is fairly common, and consists of an over-reaction to cold, where arteries of the hands constrict, and the fingers get white and cold. Burger’s disease involves small arteries, and often is associated with Raynaud’s. The arteries carry the blood distally (away from the heart), continuing to divide into ever smaller arterioles which terminate in capillaries, which branch out in such an arborization as to supply all cells except cartilage and parts of the eye.
HYPERTENSION develops when the arterioles, under hormonal or neural influence, constrict, increasing the resistance to blood flow, and so the pressure. Increase in sodium retention and therefore the blood volume can also increase pressure.
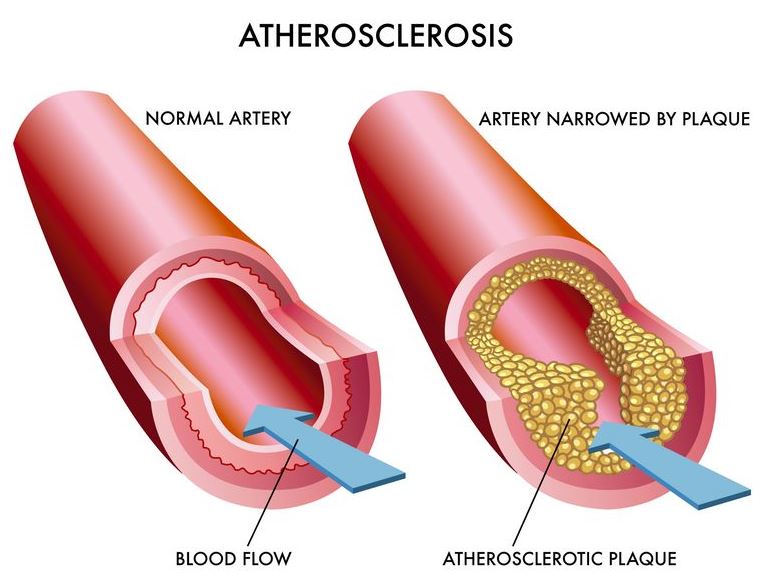
ATHEROSCLEROSIS is the common disease of western life style. Excessive calories and sedentary life style combined with genetic defects in fatty metabolism produce cholesterol plaques which narrow and stiffen the arteries, often leading to BLOCKAGE of blood flow. Blockage of flow to the HEART, BRAIN, KIDNEYS, BOWEL, or EXTREMITIES each produce their separate disorders of Myocardial Infarction, Stroke, Renal artery Disease. Intestinal ischemic syndrome, and Claudication.
These disorders will each be separately discussed. I have always thought of vascular disease as a special class of CAUSATIVE MECHANISMS when trying to develop a DIFFERENTIAL DIAGNOSIS of a patient’s problems. Blockage to an area results in PAIN or LOSS OF FUNCTION.
Stroke is usually painless with blockage, since the brain has no pain sensors. Blockage of the renal artery often causes complex difficulties including Hypertension, because the kidney is an endocrine organ in addition to its excretory function.
A good Friend and patient showed what careful self-care can accomplish. It all started with a myocardial infarction, the first sign of his blood vessel disease. He had a complication in his workup, and had to have emergency bypass surgery. There had been damage to the heart muscle, with a large reduction in his EJECTION FRACTION.
His cardiologist gave him at most 5 years to live. That was 25 years ago, before the development of the statin drugs. He was given a draconian low cholesterol diet, which he followed exactly. One one visit to the cardiologist, he inquired 
In an orthopedist office for back pain, the orthopedist left the room, and my friend noticed in the CT scan report mention of cysts in the kidneys.
The Orthopedist cared mainly about his bones, and had overlooked the “incidental finding”. His brother had died of mesenteric artery blockage from atherosclerosis, he had stomach symptoms, and sure enough he also had arterial blockage to the intestines.
Bottom line: it pays to be an ACTIVE PARTICIPANT in our medical treatment, and even though we all have genetic determinants, we can make our health BETTER with attention to our health, especially SLEEP, DIET and EXERCISE.


