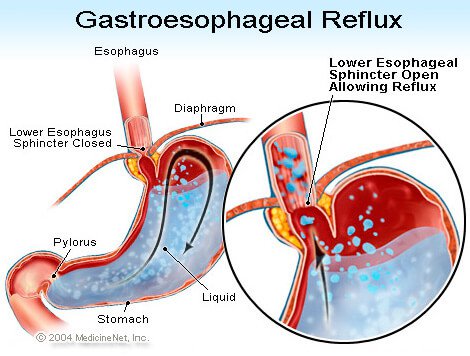
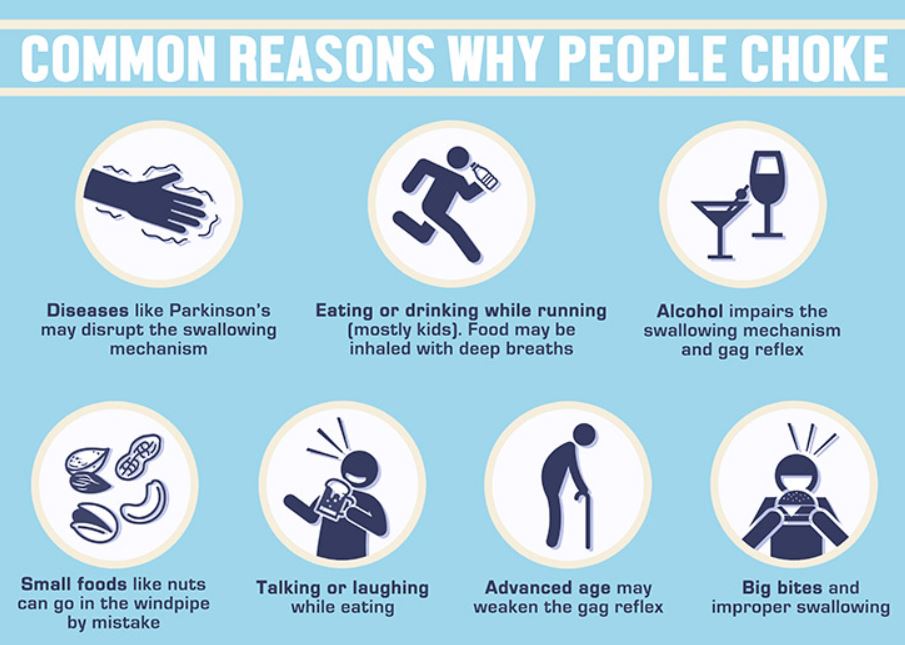
DYSPHAGIA covers a wide range of troubles, symptoms and diseases, as indicated from the excellent Infographic posted August 21, 2020. I have already discussed GERD, or trouble with the food coming back up after being swallowed.
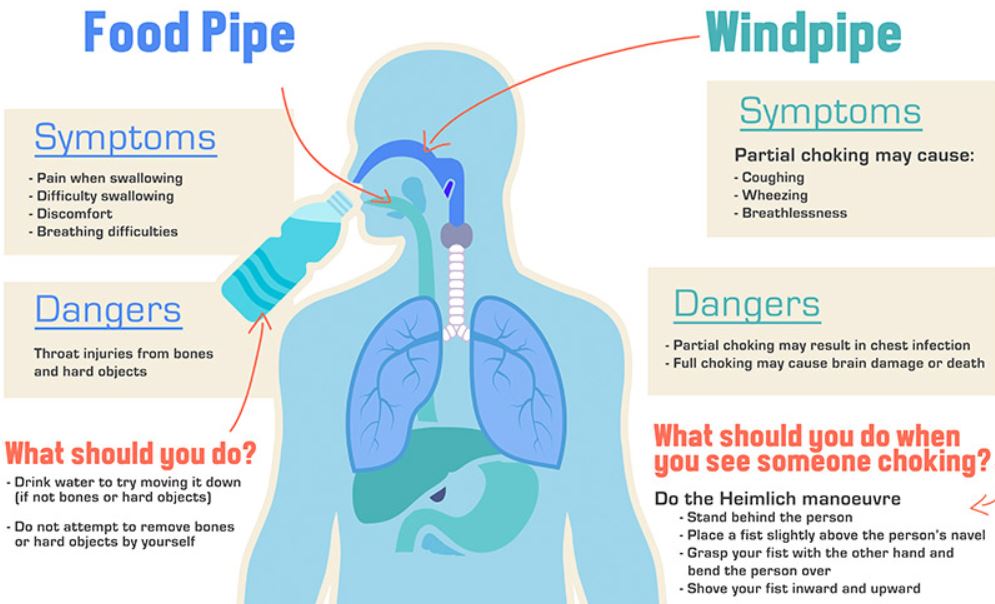
This post will be on “choking”, or getting the food into the Airway instead of the Esophagus, or swallowing tube. In the future, I will develop a post in “swallowing difficulties”, or trouble getting the food to pass easily and freely down the esophagus into the stomach.
CHEWING the food properly is rare in our rushed, fast-food society, but it is very important, the first part of the digestion process. Mastication breaks the food into smaller particles that are easier to digest, and also EASIER TO SWALLOW. Saliva flows as you chew, and contains Ptyalin, an enzyme which breaks down starch into absorbable sugars.
Chewing also SLOWS down the rate of eating, improves enjoyment, and allows more time for the stomach to send Satiety signals to the brain. This leads to less overeating and weight gain. In children, chewing is said to aid in jaw development and to reduce dental crowding and need for Orthodontia.
Some people have trouble in Initiating the swallowing process. This can be caused by neurological problems like Parkinson’s Disease. It can also be Psychological, a reflection of fear of discomfort on swallowing.
I have the opposite problem, a tendency to swallow too eagerly and rapidly, causing me to choke on liquids, sometimes even on water. I went to an ENT specializing in swallowing problems. He checked the sensitivity of my throat to touch, and found it normal.
Apparently LESSENED sensitivity is the main concern, which would
lead to Aspiration of food. The only guidance he gave me was to eat and drink more slowly. I find that I am most likely to choke when I drink wine, or a tasty beverage which I tend to “slurp” so as to fan the aroma out broadly in my mouth. I am having a hard time breaking myself of that habit.
Sometimes I find that residual amounts of food builds up in the back of my throat, probably by my epiglottis. I worry about nuts especially. If I don’t drink some water to flush it away, I am likely to choke on it. I guess that is the reason people are told to offer some water to a person who is choking.
I seem to be choking more as I get older, which is reasonable. Swallowing requires an amazingly intricate coordination and motion in the throat area, especially in getting the epiglottis, the little door that closes off the windpipe, to close properly.
My other dexterities are fading, why should swallowing be an exception? Pill swallowing is getting more frequent and more problematic at the same time.
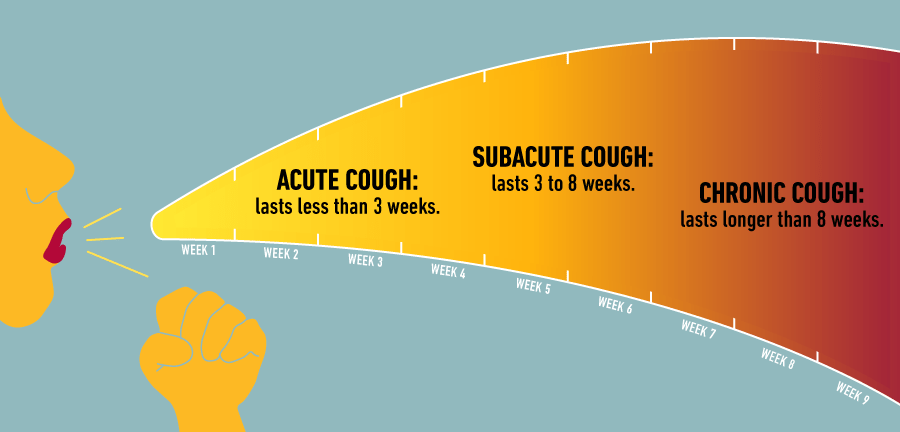
Tablets are worse than capsules, maybe because they are not as slick. There is one size in particular that tends to get stuck in the back of my throat just above the uvula. I sometimes have to cough a lot and choke the offending object back up. One more reason to constantly try to cut down the number of pills.
There is one good thing about this problem, however. I now take the pills separately with a big swallow of water, improving my Hydration.