The Journal Science recently reported on nearly 77,000 patients hospitalized with Covid 19. 29% were overweight and 48% were Obese. A total of 77% of admissions for Covid were overweight or worse.
Overweight was defined as BMI of 25-29.9 Kg. per Square Meter, and Obese was defined as BMI of 30 or greater. Another way of stating the data is giving the rate of Hospital admissions per 10,000 People.
- Normal Weight, BMI 18.5-25 kg. Per square Meter—12%
- Overweight, BMI 25-29.9 per square a Meter———-19%
- Obese, BMI 30-34.9 per square Meter——————-23%
- Severe Obesity, more than 35 per square meter——-42%
BMI calculators are everywhere to be found on the internet. Put in your weight and height, and find your BMI displayed.
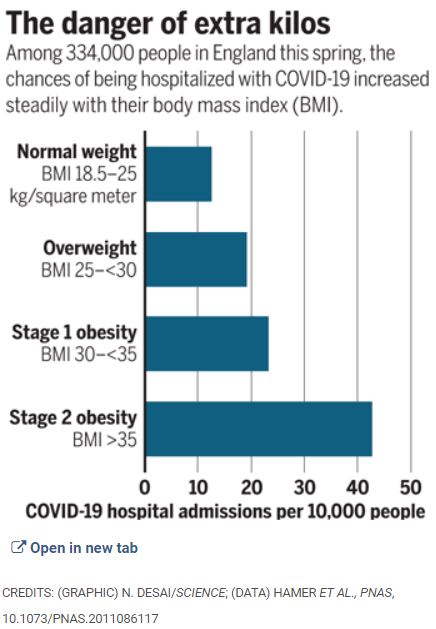
These are striking figures, the more so because of the LARGE SAMPLE, and the LINEAR Relationship; the greater the overweight, the greater the hospitalization rate.
Every way you look at it, obesity is hazardous. More hip and knee replacements, harder to exercise, find comfortable seats, more difficult to do surgery, more diabetes, heart attacks, stroke, Hypertension, Sleep apnea, worse immunity, and now, confirming previous suspicions, clearly higher risk of being hospitalized (and dying) with Covid.
I realize that nobody chooses to be Obese; in addition to the health problems, overweight people are Subjected to discrimination.
Obesity is notoriously hard to treat; one of the few, seldom mentioned medical truths is that Diets fail long term. Starting and maintaining a diet takes Herculean Will Power, which is in short supply in our overindulgent, overadvertised, and overfed society.
If I were morbidly Obese, I might opt for Bariatric Surgery, and try my best to hold the short term weight loss, since even with surgery the pounds tend to creep back on over time.
The best way to treat Obesity is to treat it as the Plague it is. CHILDHOOD OBESITY should be treated aggressively. Keep the Obese Child from becoming an obese adult, and maybe carry yourself along with the Family.
Better yet, Good SLEEP, DIET, and EXERCISE come as an interactive mutually reinforcing package deal. Prevention always beats treatment.
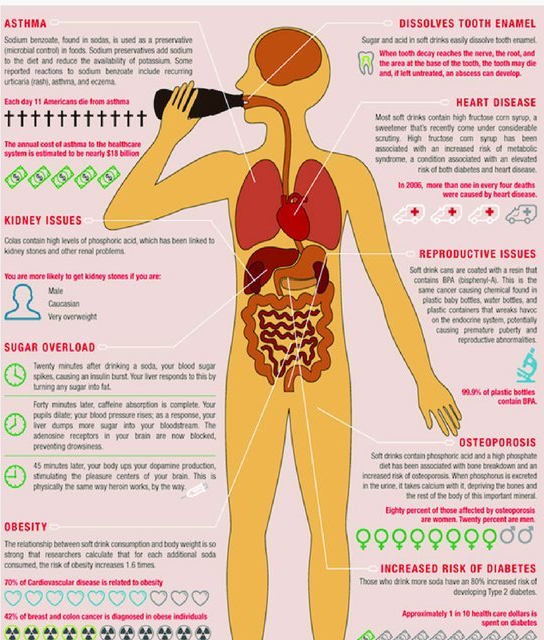
My article on ABDOMINAL FAT is suggested reading, and there is a link to the Infographic which Displays the above date in graphic form.