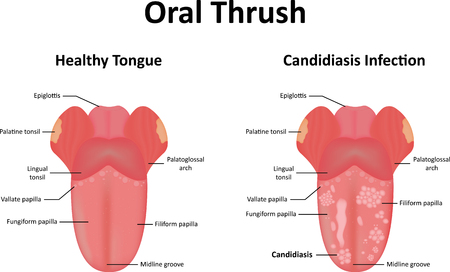
Thrush is an infection of the mouth with an organism called candida albicans. It is most common in the newborn and with young children, but can occur in adults if they have an immune deficiency, use corticosteroid inhalers, are diabetic, or take broad-spectrum antibiotics.
A combined mother–child problem can occur with breast-feeding mothers in the newborn period. The mother’s nipples may become infected, giving it to the baby, and they can pass back and forth. A baby who has thrush is also susceptible to diaper rash caused by candida.
There is a sense of irritation and some pain associated with thrush in the mouth, the diaper area, and the nipples. Thrush appears as cottage cheese-like areas on the throat and tongue.
The normal immunity usually keeps thrush at bay. In a newborn, however, the immune system is not fully developed. Sometimes the hormones of pregnancy facilitate thrush in the mother. Diabetes and smoking can also allow thrush.
Sometimes the thrush infection will go down into the swallowing tube, the esophagus, and produce inflammation. This can cause pain on swallowing, and is most common in AIDS and other immunodeficiency states.
Treatment of surface candida infections like throat is usually with Mycostatin– containing mouthwashes or creams. If it spreads beyond the surface, however, you will need more potent medications. Candida albicans is everywhere, and your immunity is your main defense against it.
Keep your immunity as solid as possible naturally, with good sleep, diet and exercise.
Painful, stiff joints are almost the rule as we get older, it seems. Both osteoarthritis and rheumatoid arthritis contribute to that eventuality. Osteoarthritis typically worsens as we get older, whereas rheumatoid arthritis starts in middle age.
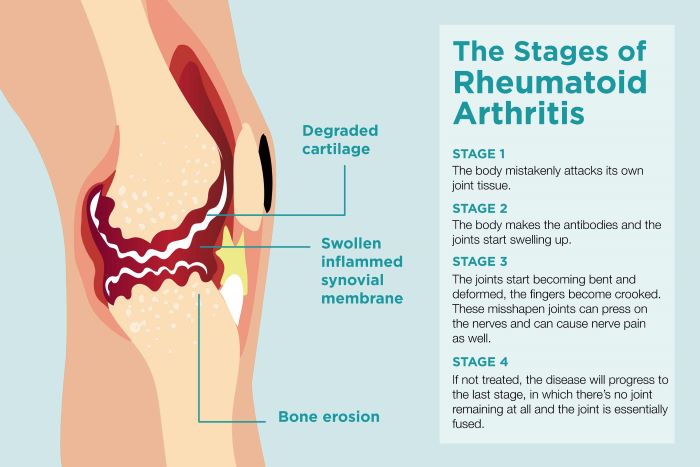
Rheumatoid arthritis is much more severe than osteoarthritis, since it is an autoimmune condition with an episodic inflammatory component. A recent medical study of different blood substances found that the “metabolome” has many markers for exacerbation of rheumatoid arthritis.
The main test currently being used to show exacerbation is CRP, C-reactive protein. Rheumatoid factor tests, such as anti-CCP, are used to confirm the diagnosis.
Rheumatoid arthritis tends to involve the small joints of the hand, and osteoarthritis the larger joints, such as the hips and knees. I go a bit against the grain, having diagnosed osteoarthritis of my fingers and toes, more typical of RA, but, even at the age of 89, my large joints are still in good shape, even with a lot of walking. Since walking is thought to increase the perfusion of joint fluid to nourish the knee cartilages, perhaps I should say BECAUSE of walking. Running tends to wear the knees and hips out, because of high impact on the joints.
The inflammation of rheumatoid arthritis tends to wax and wane, but during an exacerbation can be quite incapacitating. The interleukin TNF seems instrumental in causing these flares, and antibodies directed towards TNF, such as etanercept, has been a helpful treatment. This injection is also given for other inflammatory, autoimmune conditions such as psoriasis, particularly psoriatic arthritis, and the inflammatory bowel diseases.
Almost half the people who have rheumatoid arthritis also experience signs and symptoms in other tissues, such as the skin, eyes, heart, and lungs. It is truly a systemic, autoimmune disease.
For more information please consult the following mayo clinic article on rheumatoid arthritis.
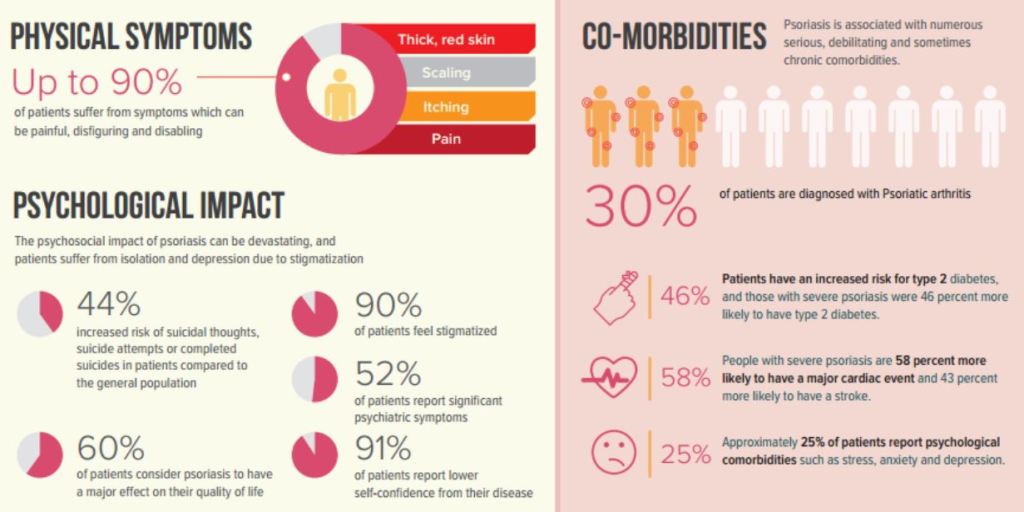
Psoriasis is a common skin disease, thought to be in the auto immune category. One of the main elements supporting auto immunity is it’s frequent association with an arthritis, which can be severe.
Eczema (atopic dermatitis) is both a skin and an allergic disease, and looks a bit like psoriasis. In my practice I saw many patients with psoriasis, perhaps people confusing allergy and dermatology.
Both psoriasis and eczema have a red inflamed base, with many little silvery scales of skin on top. These patchy areas tend to be on the outside bends of the elbows and knees in psoriasis, contrasting with eczema, where the dermatitis is located on the inside of the bends. Eczema is a lot more itchy.
The cause of the skin lesions in psoriasis is thought to be due to an interleukin called TNF, which calls to the area a number of inflammatory cells which, in addition to the thickened skin area and excess of epithelial cells, leads to a characteristic appearance under the microscope; biopsies are uncommonly needed when there is doubt about the diagnosis.
In its severe form, psoriasis can be very disfiguring, irritating, painful or itchy, and life altering. You have probably seen advertisements on TV. Psoriasis has accumulated many different treatments, since it has been recognized and treated over such a long period of time. The basis of many effective treatments is “shotgun” systemic immunosuppression, which reduces the autoimmune inflammatory reaction, but with side effects.
Topical Cortisone cream is the cheapest reasonably effective treatment, and works for mild cases. More recent treatments are specifically aimed out the interleukins which cause the disease, like TNF.
Please refer to the mayo clinic article for more pictures, and discussion of treatment.
Hashimoto’s thyroiditis is the most common cause of thyroid deficiency. As a practicing allergist, I would routinely palpate the front of the neck area around the windpipe where the thyroid is located. Every few months or so, I would feel an enlarged thyroid, order a high sensitivity TSH test, and, if positive, check for thyroid antibodies.
This saved my patients from having to go through the symptoms of underactive thyroid(hypothyroidism), since I detected the problem at an early stage, before symptoms developed.
Major symptoms of an underactive thyroid include fatigue, increased sensitivity to the cold, constipation, unexplained weight gain, and depression. Be sure to seek medical care if you are suffering from these symptoms.
An elevated LDL cholesterol is one of the biochemical results of hypothyroidism, and can lead to heart problems. I have been hearing that the routine physical examination it is becoming less common, and may even be replaced by telemedicine. The early detection of Hashimoto’s thyroiditis will be one of the casualties, since the doctor can’t find an enlarged thyroid unless she palpates for it.
You might wonder why an enlarged thyroid gland is associated with decreased thyroid production. The way it works is that the pituitary gland at the base of the brain detects a decrease in thyroid production. It responds by secreting a thyroid stimulant, TSH. The TSH causes enlargement of the thyroid gland, leading to the association of an elevated TSH with decreased thyroid activity.
Hashimoto’s is one of the large number of autoimmune diseases. A person who has an autoimmune disease, such as rheumatoid arthritis, type one diabetes, or celiac disease, is more likely to develop others, and should be alert to that possibility.
Finding that you have low thyroid activity is only part of the problem. It takes several visits plus input from both patient and doctor in order to arrive at the proper medication schedule. There are several different thyroid medications, and people respond differently to them.
Be on the alert for hypothyroidism. It can sneak up on you.
When not walking barefoot at night or on the beach, my toes have been squeezed together most of my life. Closed-toe compression stockings for my varicose veins plus inadequate space at the front of my shoes have encouraged my big toe to “scissor” and to cross over the second toe. At that point I started wearing open-toe stockings, and tried to give my toes more room in larger shoes. I also used a spacer to push the big toe out.
Walking on the beach is a wonderful place to free up your toes. For a while, I walked in the deep sand at the top of the beach, trying to get more exercise. Periodically I would get some thorns in my feet, and go to podiatrist to get them out.
During one visit, the podiatrist told me that I was getting a hammer toe in the toe right next to my big toe, and I now use a little ring shaped cushion for that second toe, incorporated with a spacer.
It is amazing how little we use the musculature of our feet, and how surprisingly well they hold up. People that are really in good athletic shape stress flexibility as being very important, and athletes often do stretching exercises before they do their workout. Practically anything that will stretch a joint is helpful, such as flexing, extending, and spreading the toes, plus flexing and extending the foot.
You can overdo it, however, as I have learned to my discomfort. You must do any exercise within the limitations of your body, beginning slowly, and working up to your desired level.
My big toe has almost no flexibility, and the joint that attaches it to the foot is enlarged and pretty fixed. I am very careful how much range and pressure I use .Even something as simple as stretching the Achilles tendon can be a problem if you do too much of it all at once. Always work slowly into your exercises to make sure that you do no harm.
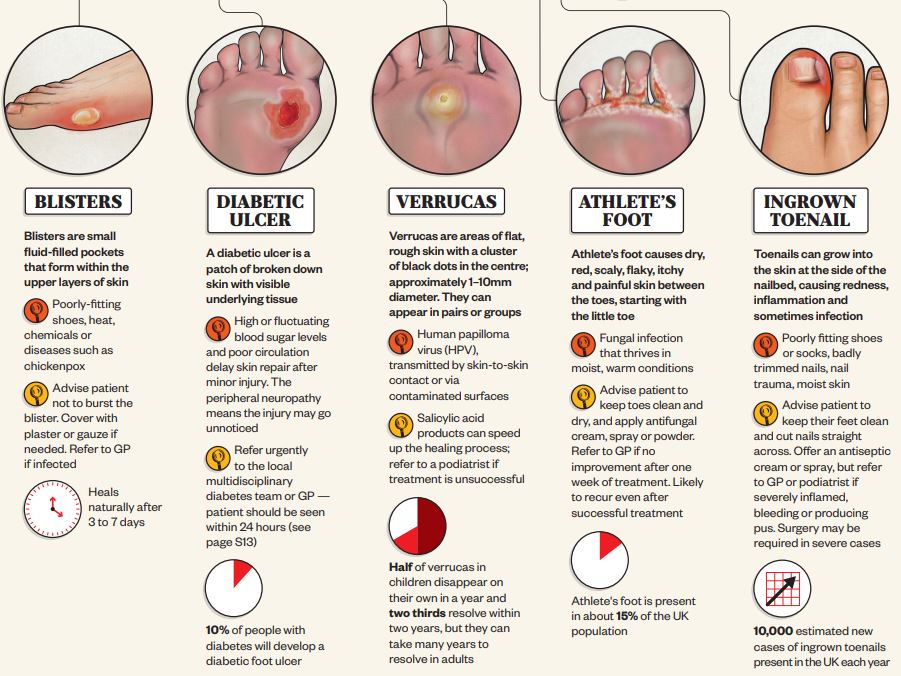
Ingrown toenails have also bothered me from time to time. I very carefully try to trim them back and avoid breaking the skin; the foot is easily infected, particularly among diabetics and older people. A podiatrist is very helpful if you let things go too far.
My toenails, particularly on my big toe, are getting white and thick with a nail fungus. This can be treated with an oral medication, dispensed by a doctor or a podiatrist. I have chosen to keep it in check with clotrimazole cream, and that seems to be working. I worry from time to time about creating a resistance factor in the fungus, but they are very slow growing, and not likely to develop a mutation.
If you would like further discussion on foot exercises, please check the following reference, one of many on the Internet.
In a very good article, the Journal ‘Science’ has collated a lot of basic science regarding aerosol transmissions in viral infection generally, and Covid-19 in particular.
Early in the epidemic, I thought that large droplet transmission, which fell to the floor, and was transmitted by fomites and hand autoinoculation into the respiratory membranes, was more important. The main thesis of the article is that it is not large droplets, but aerosol particles that mainly transmit.
The secondary assertion is that aerosols can be up to 100 µm microns in diameter and still be transmitted by inhalation. they also stated that particle size of equal or less than 5 µm contain more virus particles than all the larger particles put together in spite of the greater mass of the larger particles . Normal speaking creates about 1000 aerosol particles per minute, And normal breathing about 7200 aerosol particles per liter of exhaled air. Coughing is more sporadic and tends to produce the larger droplets which don’t stay airborne as long, but I wouldn’t count on it.
There is a tremendous difference between individuals as to the number of particles they generate. It’s estimated that 10 to 20% of individuals account for 80 to 90% of the virus.
Slide number two deals with viral load and infectivity which is a function of the pH value, electrical charge, and other characteristics of the virus. An important point is that even though there is lots of viral RNA, that doesn’t mean that the virus is infective. Once again there’s a tremendous difference between the infective viable virus content of the aerosols from infected patient to patient. He stated that in one room with two Covid patients, they were 6 to 74 TCID/50 per liter, which means you’re almost certain to be infected if you don’t have a mask that filters out the virus, or some kind of purification in the room.
Slide Three was very interesting to me. The persistence in hours graphed against the aerosol particles size. 100 µm particles stay in the air only about five seconds, 5 µm particles stay in the air for 30 minutes, and one micrometer particles will stay in the air for 12 hours or more.
The fourth slide talks about factors affecting the distribution of indoor aerosols. There may be certain parts of the room where the particles congregate , depending on the ventilation type, whether natural, mechanical or filtered, flow patterns within the room, and indoor filtration and killing devices such as ultraviolet light.
Mention is made of the CO2 level in the room as a measure of air circulation. There is a higher CO2 in the air with lots of people and poor ventilation. The recommendation is that 7-8 ppm is about the highest acceptable level, and the possibility of using a portable HEPA filter would not be a bad idea for people frequenting indoor restaurants. Of course, outdoor air with its breezes, dispersion, less humidity, higher ultraviolet and usually Greater dispersion of people is preferable to indoor contact.
Some other interesting points are that children produce less aerosol particles because they have a smaller number of bronchi. I thought the bacteria were less likely to be aerosol transmitted than viruses, but they state that the R0 of tuberculosis can be as high as 4.3, vs. 7-8 for covid. The typical tuberculosis bacillus is relatively large, and yet is only 2 µm in length, well within the size of an aerosol particle.
–Dr. C
Empowering Patients Through Education And Telemedicine