

DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING SEPTEMBER 14, 2020.
Category Archives: Opinion

COVID-19 STUDIES: 77% OF HOSPITALIZED PATIENTS ARE OVERWEIGHT OR OBESE

The Journal Science recently reported on nearly 77,000 patients hospitalized with Covid 19. 29% were overweight and 48% were Obese. A total of 77% of admissions for Covid were overweight or worse.
Overweight was defined as BMI of 25-29.9 Kg. per Square Meter, and Obese was defined as BMI of 30 or greater. Another way of stating the data is giving the rate of Hospital admissions per 10,000 People.
- Normal Weight, BMI 18.5-25 kg. Per square Meter—12%
- Overweight, BMI 25-29.9 per square a Meter———-19%
- Obese, BMI 30-34.9 per square Meter——————-23%
- Severe Obesity, more than 35 per square meter——-42%
BMI calculators are everywhere to be found on the internet. Put in your weight and height, and find your BMI displayed.
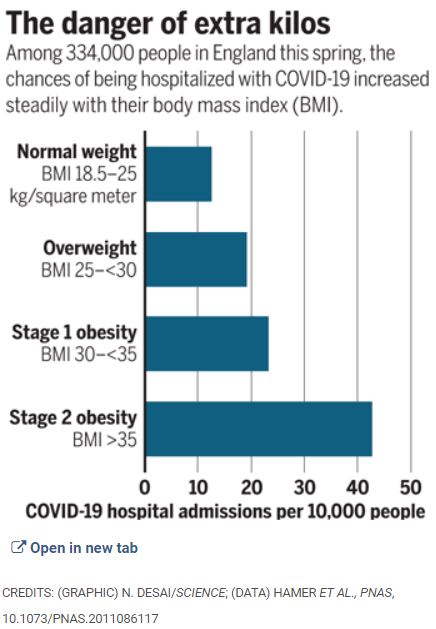
These are striking figures, the more so because of the LARGE SAMPLE, and the LINEAR Relationship; the greater the overweight, the greater the hospitalization rate.
Every way you look at it, obesity is hazardous. More hip and knee replacements, harder to exercise, find comfortable seats, more difficult to do surgery, more diabetes, heart attacks, stroke, Hypertension, Sleep apnea, worse immunity, and now, confirming previous suspicions, clearly higher risk of being hospitalized (and dying) with Covid.
I realize that nobody chooses to be Obese; in addition to the health problems, overweight people are Subjected to discrimination.
Obesity is notoriously hard to treat; one of the few, seldom mentioned medical truths is that Diets fail long term. Starting and maintaining a diet takes Herculean Will Power, which is in short supply in our overindulgent, overadvertised, and overfed society.
If I were morbidly Obese, I might opt for Bariatric Surgery, and try my best to hold the short term weight loss, since even with surgery the pounds tend to creep back on over time.
The best way to treat Obesity is to treat it as the Plague it is. CHILDHOOD OBESITY should be treated aggressively. Keep the Obese Child from becoming an obese adult, and maybe carry yourself along with the Family.
Better yet, Good SLEEP, DIET, and EXERCISE come as an interactive mutually reinforcing package deal. Prevention always beats treatment.
My article on ABDOMINAL FAT is suggested reading, and there is a link to the Infographic which Displays the above date in graphic form.
—Dr. C.

DR. C’S MEDICINE CABINET: BENEFITS OF “FINASTERIDE”
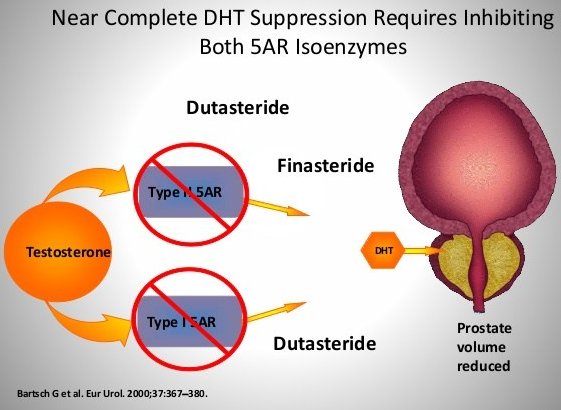
Finasteride is a medication that I was given by my urologist, after my operation for an enlarged prostate with restricted urine flow. It was used to prevent the re-growth of the prostate, and subsequent recurrence of urinary obstruction.

It is also recommended to treat male-pattern baldness. That it is used to treat male problems suggests that it has something to do with testosterone, and indeed it does. Finasteride (proscar) is a 5-alpha reductase inhibitor, preventing testosterone from being converted to dihydrotesterone, the active form, in the prostate and the skin.
Finasteride is well studied, and has been found to decrease PSA in the blood, and is suspected of interfering with the use of PSA as a screening device for Prostatic Cancer. It has also been suspected of increasing severe, high grade cancer. These findings have been refuted in later papers.
It has also been found to decrease sexual function, which it has in my case. I have continued it for several reasons.
First, my urine flow remains fine. Second, the bulk of the data indicates that it hinders prostatic cancer formation; and in a previous posting, I stated that Prostatic cancer in 88 year-olds is almost universal. Third, we are continuing in a Covid 19 pandemic.
One of the markers for severe infection is male-pattern baldness, which finasteride prevents. I did find in my reading about finasteride that there is a 1 mg. dose, and I am taking 5 mg..
When the Covid epidemic slows, I will probably opt for the 1 mg. Dose, which produces a significant effect, though of course less than the 5 mg. Less medication is usually better.
For Patients with BPH opting for medical treatment, Finasteride is usually recommended along with an alpha adrenergic agonist to relax the bladder sphincter.
For the men out there, facing an ever-increasing likelihood of BPH, or wanting to slow down baldness, you may eventually be making the decision whether or not to take this effective medication.
–Dr. C.

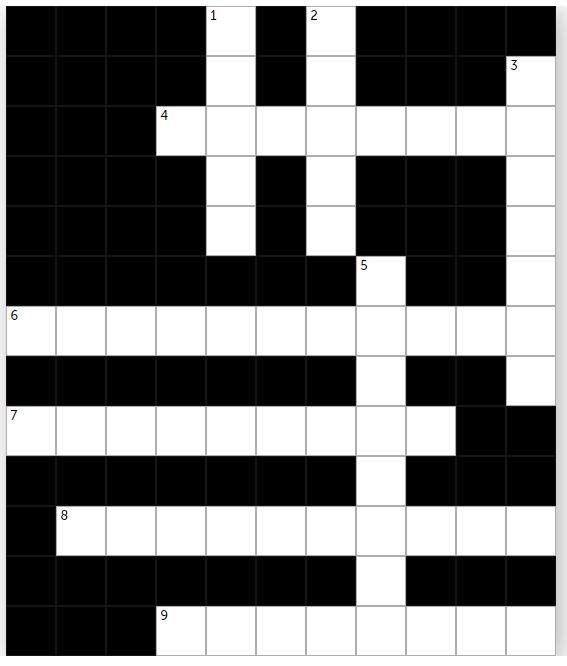
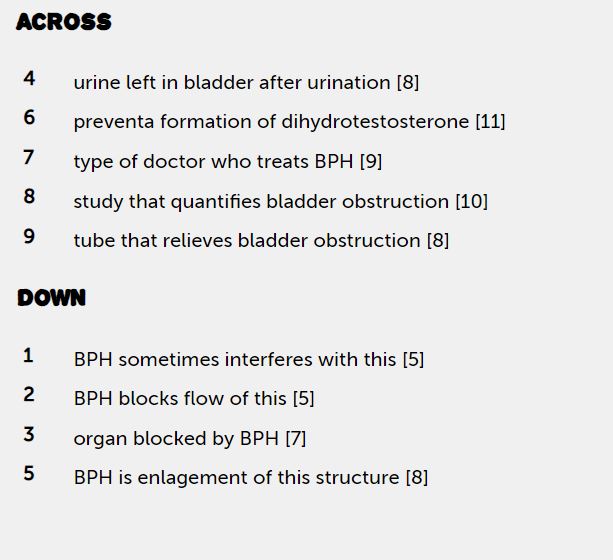
PATIENT EDUCATION: THE “2020 WEEKLY CROSSWORD PUZZLE CHALLENGE” (SEPT 8)
DR. C’S PODCAST: WEEKLY MEDICAL NEWS (SEPT 7)
DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING SEPTEMBER 7, 2020.

THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #14: TRIGEMINAL NEURALGIA
My Mother had Tic Douloureux, the traditional name for Trigeminal Neuralgia. I remember her suddenly covering her face with her hand and grimacing, but this was only occasionally.
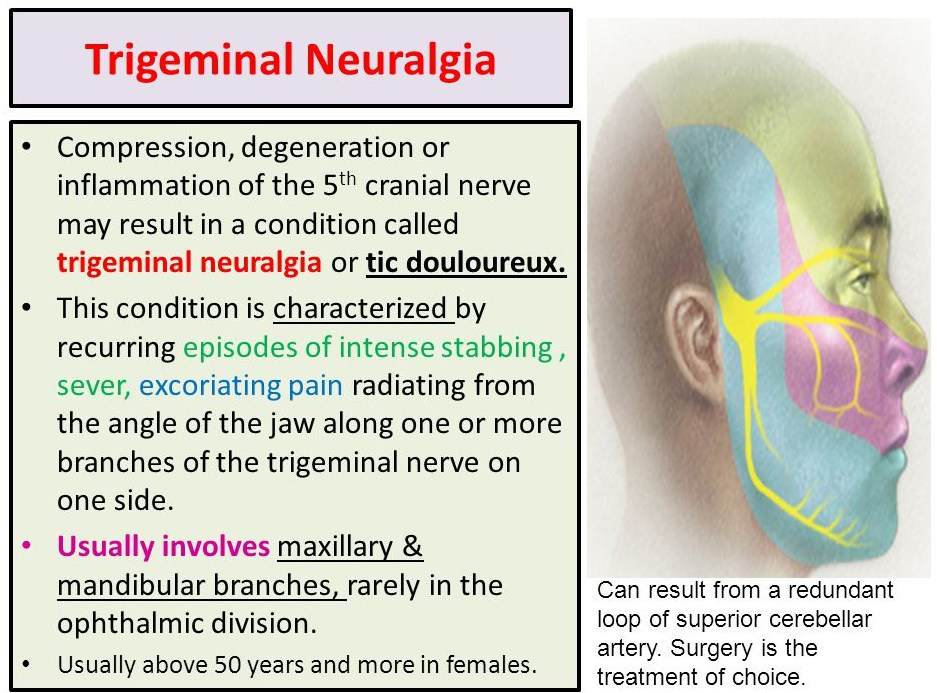
TD is not very common for “101 chronic conditions”, but it is the most common cause of chronic facial pain. It occurs in the FACIAL region supplied by the 5th cranial, or TRIGEMINAL nerve. This is about the area covered by your widely spread hand, pinkie on the nose, and the butt of the palm along the jawbone.
Brief shocking pain occurs in “PAROXYSMS” in the facial area, on ONE SIDE, and TRIGGERED by tooth brushing, touching the face, or even by the blowing of the wind. This description is so typical and specific as to be “pathognomonic”, and can be diagnosed over the telephone.
Variants can give continuous pain, or occur on both sides, but the “classical” variety is most common. You should contact your Doctor, since some cases are caused by Multiple Sclerosis or a tumor. Effective medications are available, such as carbamazepine.
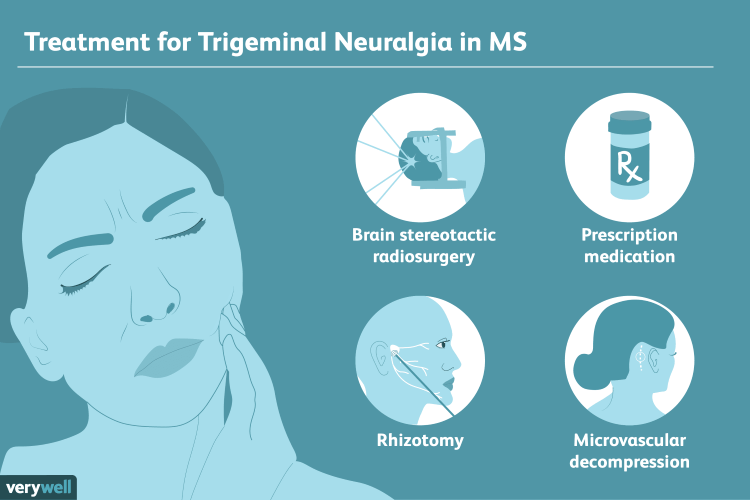
TD can be familial, but is often caused by compression of a nearby artery, and “decompression” is currently the most effective surgical treatment. It is one of the few “chronic 101” conditions not to be substantially prevented or helped by our old standbys, sleep, diet and exercise.
That being said, it is sometimes helped by exercise, and almost never occurs during sleep. The August 20, 2020 New England Journal of Medicine Has an excellent Review article, which will be appended to this posting.
–Dr. C.
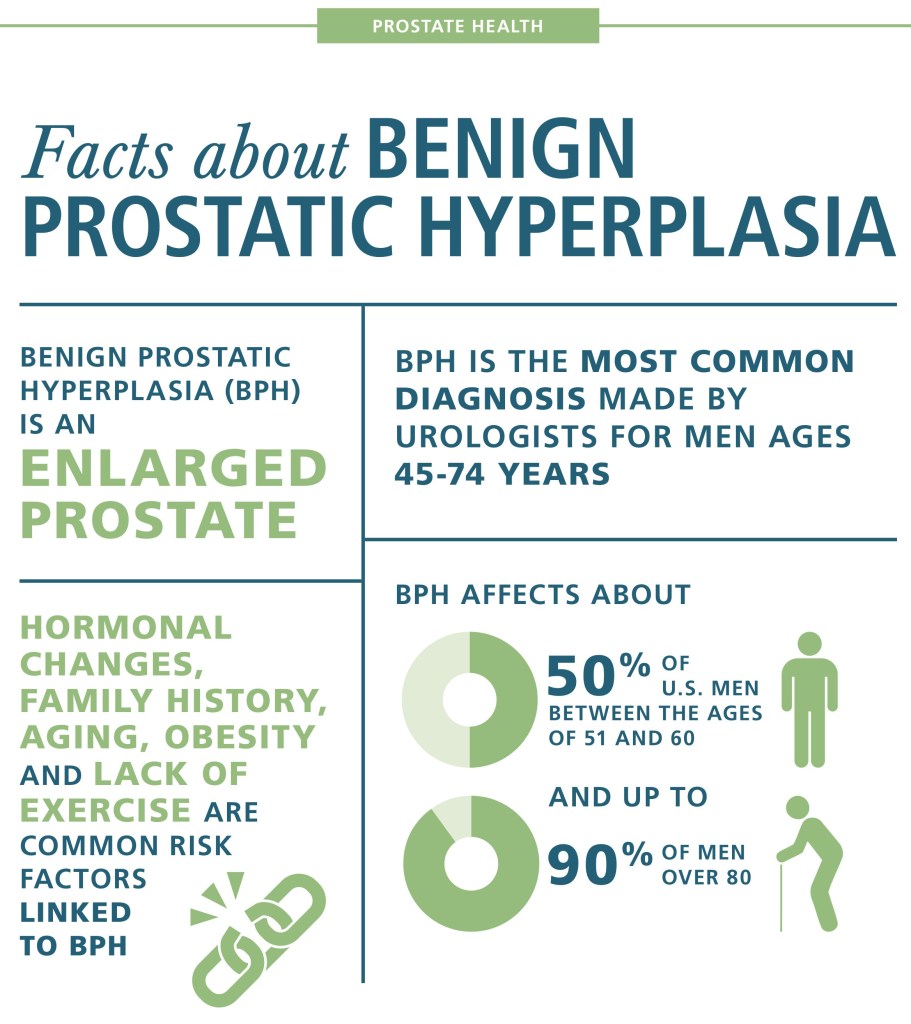
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #13: “BENIGN PROSTATIC HYPERPLASIA” (BPH)
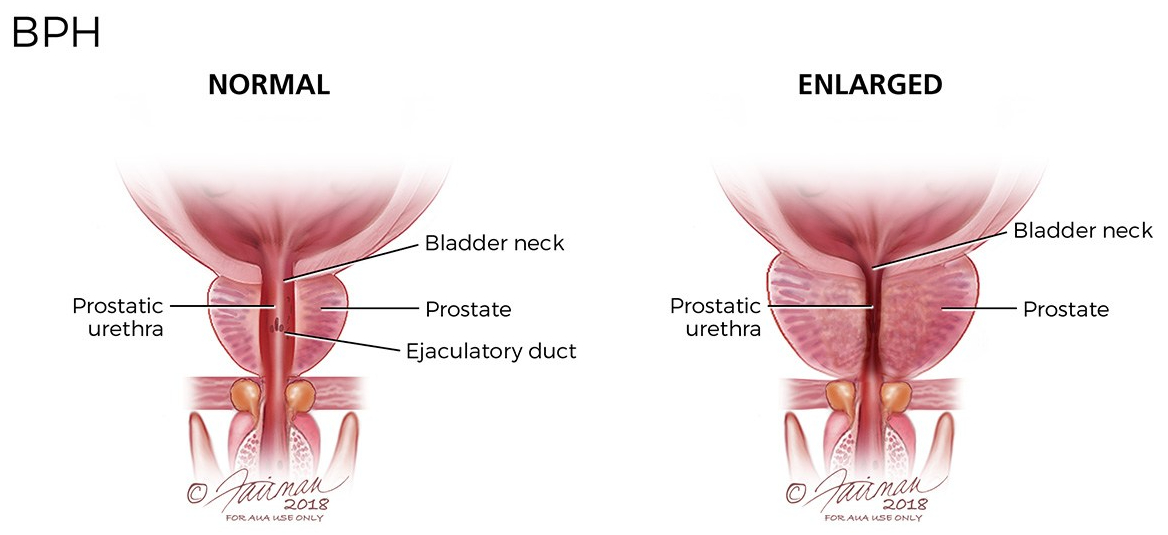
I have known about the Prostate gland, which surrounds the urethral channel exiting the bladder, since med school. I have seen evidence of its enlargement in the increasing time it takes older men to empty their bladders.
When my dad had his prostate surgery, he said that he could blast the porcelain right off the toilet, I could then appreciate for the first time that enlargement of the prostate caused a weak urinary stream.
When I started waking up at night 3 or 4 times to urinate, it really hit home. I had to get something done. My Urologist was a very good one, like all of my doctors. As the old saying goes, the best is none too good when it comes to your health.
On my first visit, he ordered a “Urodynamic” study. In this test, done by a visiting nurse who had the equipment, a small catheter, or tube, ws passed into my bladder, after loading myself with water until I could hold it no longer. The pressure in my bladder was measured, the speed with which I evacuated my bladder was measured, the volume of urine I passed was measured, as well as the volume retained in the bladder.
With these numbers, my bladder volume, residual, and the resistance to flow was calculated. I was shown to have a small bladder, too much residual retained after I emptied it, and an excessive resistance to the flow of urine out of the bladder.
I have not seen the urodynamic studies mentioned in the modern workup of BPH, and it may not have been critically necessary. I did appreciate his thoroughness, however, and factored in the study when he gave me the options of medicine vs. surgery.
were two medicines mentioned, an alpha adrenergic agonist, and finasteride, an anti-androgen. Since I would have to take both meds the rest of my life, I chose surgical enlargement of the urinary passage through the prostate, known technically as a “roto rooter job”. I, too, noticed the power of my urinary stream after the surgery.
A good friend of mine, also a physician, took medicines for many years, in spite of increasing trouble urinating, getting up at night, and frequent bathroom trips during the day. He eventually went to see a urologist after he had to go to the ER for completely being unable to pass urine.
The Urologist declined to do surgery on the basis of his health, the unusually large size of the blockage, and degree of obstruction. He used a catheter to relieve himself several times a day for the rest of his life. Had I been in his shoes, I would have tried to find a willing surgeon somewhere, perhaps at a university med school.
But then again, I wouldn’t have waited so long. These days many more options are available, and the appended article discusses some of them. –
–Dr. C.
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #12: “Prostate cancer”
Prostate cancer is perhaps the most common cancer in men. It increases in incidence with age, and if you live long enough, most men will contract prostate cancer. A family history of cancer and obesity are also risk factors. But many times the cancer is so slow growing that it will not kill you. In the age of modern, aggressive medicine, the treatment has often been worse than the disease.
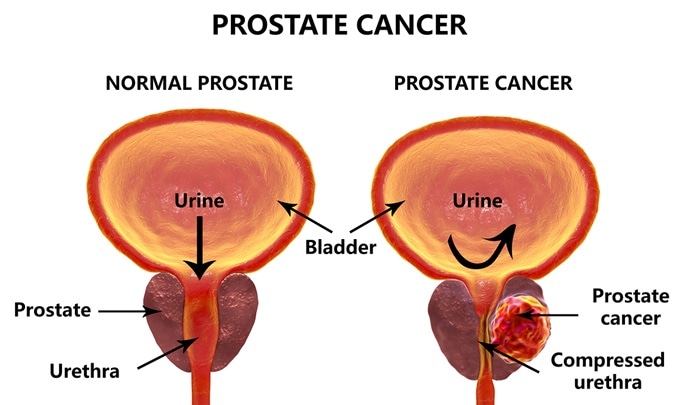
Treating Cancer EARLY is much more successful. The PSA test was one of the first really sensitive blood tests for cancer, and it was once performed routinely, on a yearly basis, usually at the time of your annual physical.
The PSA (Prostate-Specific Antigen) test is VERY sensitive,however. In responding to an elevated PSA, very slow growing tumors would often be treated aggressively, creating more morbidity than the untreated tumor would have caused.
The treatment seemed to be worse than the disease. Many physicians stopped doing the PSA test altogether, relying on symptoms, or detecting an abnormality on RECTAL EXAM to trigger an investigation. Some years ago, a physician friend of mine elected to stop PSA testing, and two years later was discovered to have METASTATIC Prostate cancer. It had already spread to his bones, and he eventually died of that cancer.
This encouraged me to continue with PSA screening, though it is still considered optional. Very recently, a test has been developed which I think tips the scales back toward annual PSA testing. EXOSOMES are little (10-120 nm.) particles that effuse from many cells, especially cancer cells.
They contain a variety of DNA, RNA, proteins and lipids which allow the cells to communicate with one another. Recently, a company, ExoDx, was created to take commercial advantage of Exosomes in the diagnosis of various diseases, by testing body fluids.
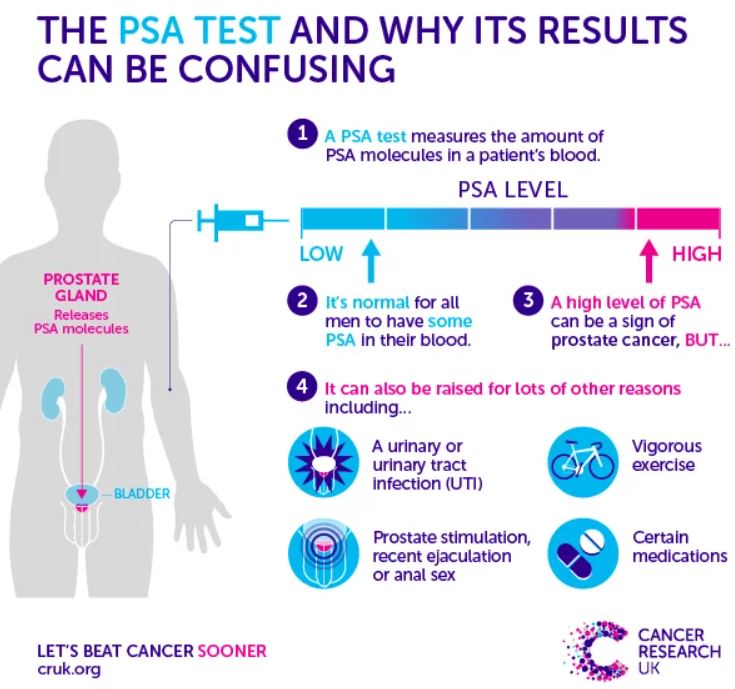
Their test, ExoRx Prostate EPI test of urine, has been shown to be helpful in distinguishing AGGRESSIVE prostate cancer from the slower growing kind, when the PSA test is in the “grey zone” between 2 and 10 ng/ml. PSA test results above 10 ng. were always acted on, especially if the numbers were increasing. I would be surprised if the PSA did not reenter the annual testing protocol.
The annual digital rectal exam in men older than 50 years will continue to be done, although it is not very sensitive, and is often not abnormal until the cancer is more advanced. Pain in the prostate area, blood in the urine or semen, and trouble urinating are symptoms worth investigating, but if cancer is detected, it may well be advanced and harder to treat. With abnormal tests,
Risk factors or suspicious symptoms, further testing is often done. Ultrasound or biopsy may be indicated. Sometimes the biopsy is guided by MRI, to increase the likelihood that the cancer, if small, is included in the tissue sample taken. Examining the cells of the biopsy sample will yield a “gleason score” which grades the aggressiveness of the cancer.
This in turn dictates the treatment, which may include different extents of surgical removal, radiation, hormonal or chemotherapy treatment. None of this is pleasant, and you are better off, of course with prevention.
Our old friends, DIET AND EXERCISE are thought to be helpful. Although not proven, eating lots of fruits and vegetables, and maintaining a healthy weight are recommended.
–DR. C

DR. C’S PODCAST: WEEKLY MEDICAL NEWS (AUG 30)
DR. C REVIEWS MAJOR HEALTH AND TELEMEDICAL NEWS FOR THE WEEK ENDING AUGUST 30, 2020.
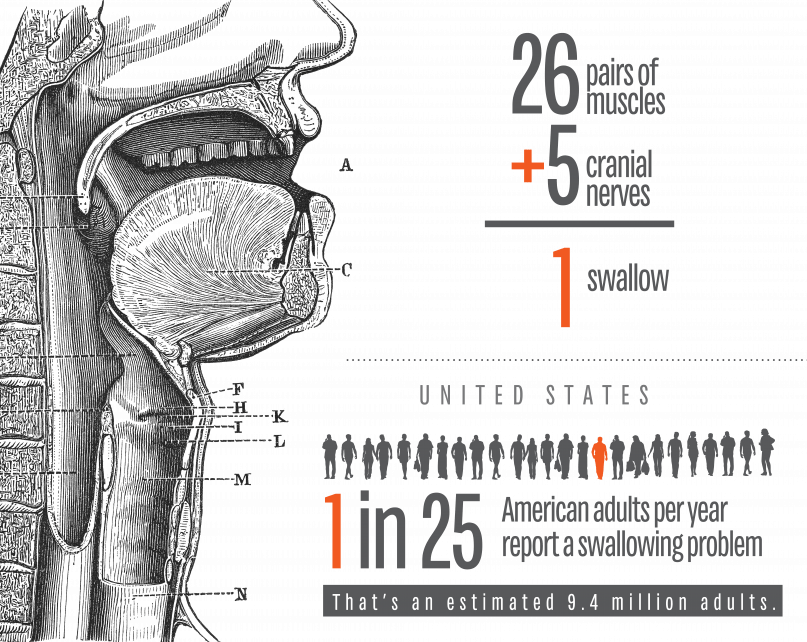
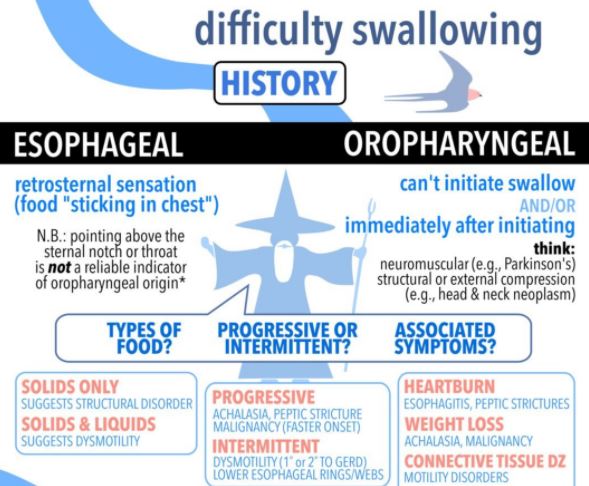
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #11: “SWALLOWING TROUBLE”
I am defining SWALLOWING TROUBLE as the difficulty in transport of food to the stomach, once clear of the throat. Problems with the initiation of the swallowing process are discussed separately.
PAIN in the mid-chest ON SWALLOWING is a worrisome symptom which can be due to inflammation of the lining of the esophagus from a variety of causes. An esophageal yeast infection, which can also involve the throat (called ‘“thrush”), often warns of immune deficiency and can be a sign of AIDS, or be caused by immune suppressing medication. If persistent, pain on swallowing can be a warning sign of CANCER.
If in the presence of GERD, it can be a sign of chronic inflammation or ulceration. In-coordination of the normally smooth muscular propulsive wave can cause a cramping, muscular pain.
Normal “peristalsis” is so efficient, that food can be swallowed without the help of gravity, when UPSIDE DOWN. I wouldn’t recommend trying this, even to cure hiccoughs. There is a muscular “gate” at the bottom of the esophagus, just as it enters the stomach. This gate is often too relaxed, and allows for the reflux of acid and food from the stomach, or GERD. It can also Fail to open, called achalasia, and hold up the food in its journey to the stomach.
The area can be scarred by repeated acid reflux, and become NARROWED; this is called a STRICTURE, and can cause a blockage in swallowing. One of my Doctor friends had to go to the Emergency room when some Steak got stuck in the esophagus.
The ER Doctor removed the steak with a fiberoptic Scope, and then proceeded to DILATE the stricture with a “bougie”, an instrument of a precisely calibrated size designed to STRETCH the constricted area. This uncomfortable procedure had to be done repeatedly, a caution to those who would wait too long before getting such a problem evaluated and corrected.
EOSINOPHILIC ESOPHAGITIS has been diagnosed with increasing frequency, and can cause Pain in the middle of the chest, trouble swallowing, and even regurgitation of food. This special type of inflammation is more common in allergic patients, and can be caused by certain foods.
So as you can see, swallowing trouble, if persistent, is nothing to fool around with, and should be checked out by a competent doctor. Don’t wait too long.
