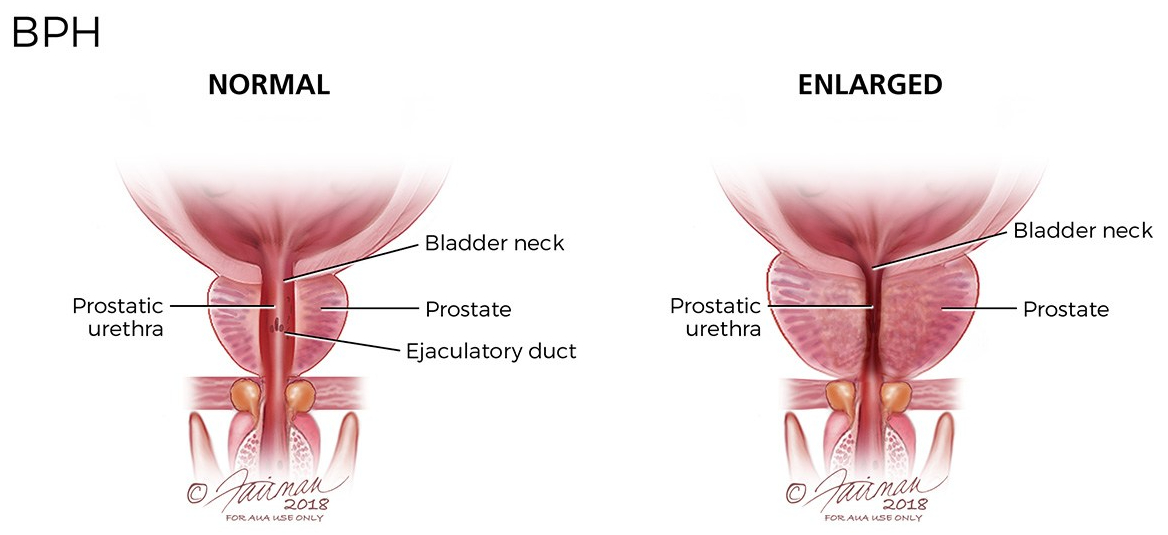
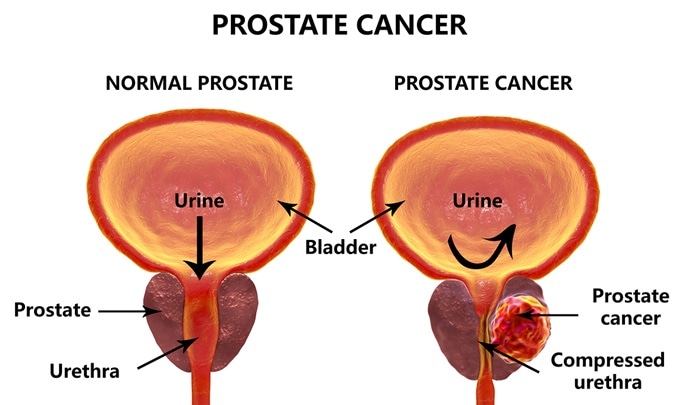
Finasteride is a medication that I was given by my urologist, after my operation for an enlarged prostate with restricted urine flow. It was used to prevent the re-growth of the prostate, and subsequent recurrence of urinary obstruction.

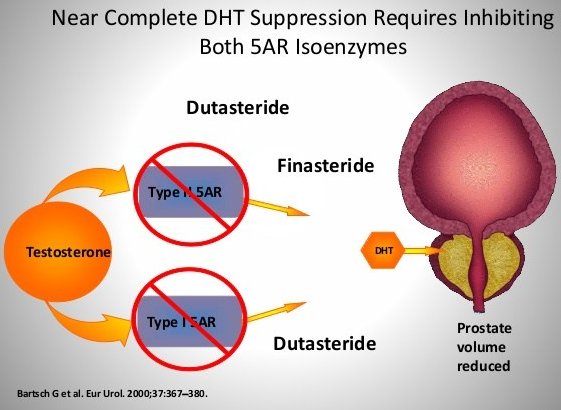
It is also recommended to treat male-pattern baldness. That it is used to treat male problems suggests that it has something to do with testosterone, and indeed it does. Finasteride (proscar) is a 5-alpha reductase inhibitor, preventing testosterone from being converted to dihydrotesterone, the active form, in the prostate and the skin.
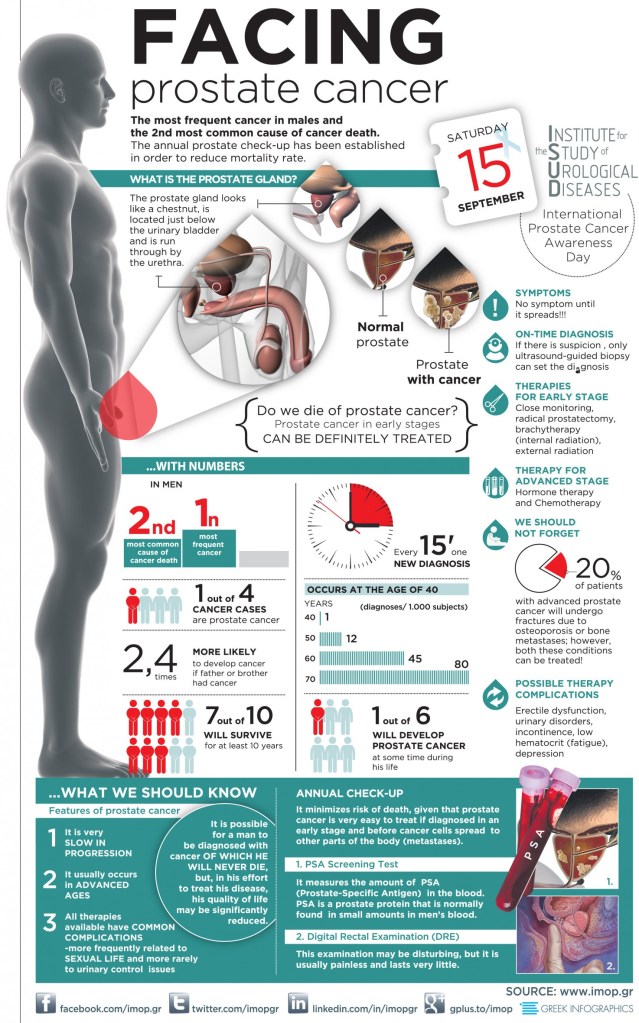
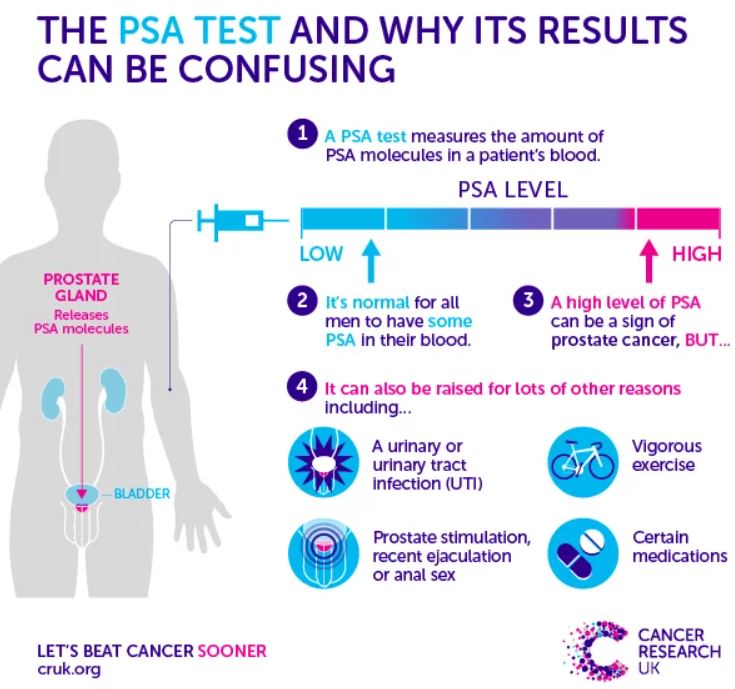
Finasteride is well studied, and has been found to decrease PSA in the blood, and is suspected of interfering with the use of PSA as a screening device for Prostatic Cancer. It has also been suspected of increasing severe, high grade cancer. These findings have been refuted in later papers.
It has also been found to decrease sexual function, which it has in my case. I have continued it for several reasons.
First, my urine flow remains fine. Second, the bulk of the data indicates that it hinders prostatic cancer formation; and in a previous posting, I stated that Prostatic cancer in 88 year-olds is almost universal. Third, we are continuing in a Covid 19 pandemic.
One of the markers for severe infection is male-pattern baldness, which finasteride prevents. I did find in my reading about finasteride that there is a 1 mg. dose, and I am taking 5 mg..
When the Covid epidemic slows, I will probably opt for the 1 mg. Dose, which produces a significant effect, though of course less than the 5 mg. Less medication is usually better.
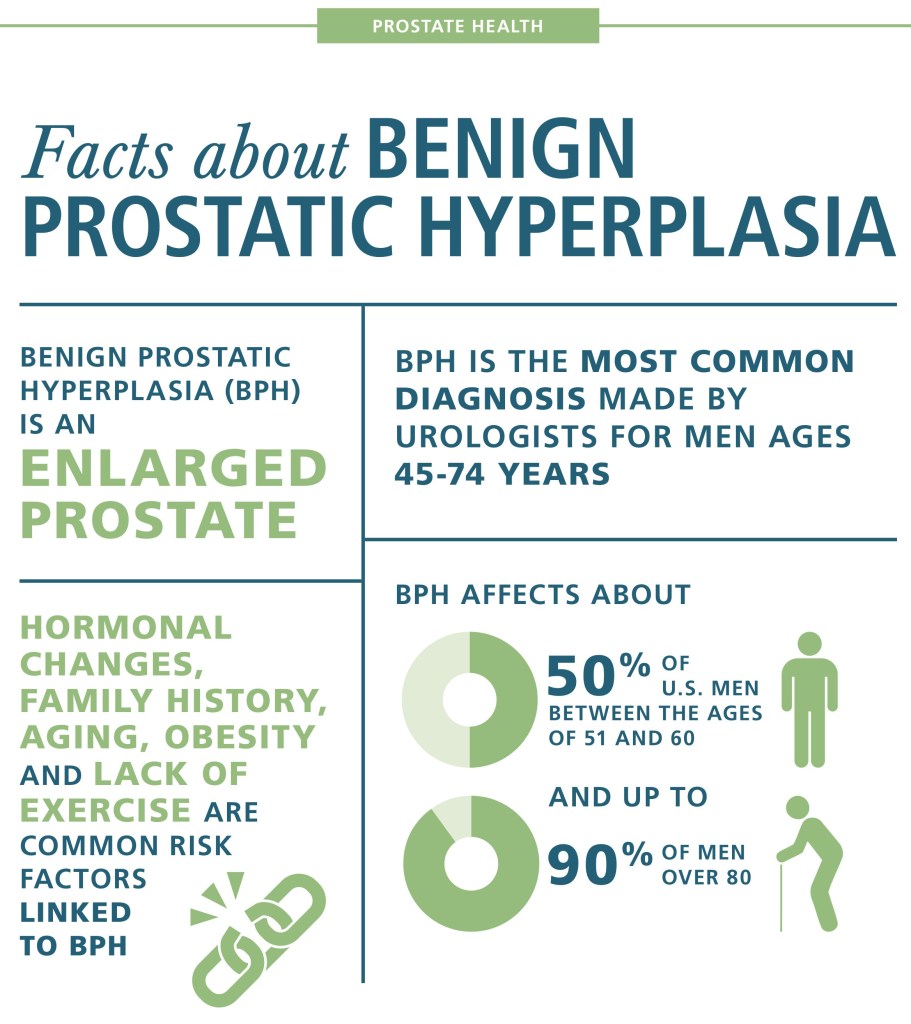
For Patients with BPH opting for medical treatment, Finasteride is usually recommended along with an alpha adrenergic agonist to relax the bladder sphincter.
For the men out there, facing an ever-increasing likelihood of BPH, or wanting to slow down baldness, you may eventually be making the decision whether or not to take this effective medication.






 Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.
Finasteride, one of the drugs in my medicine cabinet is mentioned as a possible aid. I will be discussing this later. I suggest that you press the green box with the magnifying glass, and type the name of the drug to see if i have discussed it. –Dr. C.