

Ever wondered what it might be like to have your own personal coach to help you live a healthier life? In many ways, this is what cardiac rehab (#cvRehab) programs do for people recovering from certain heart-related conditions and procedures 👉 https://t.co/onuN586B9h pic.twitter.com/pDEqBpLOfh
— CardioSmart (@CardioSmart) July 13, 2021
Category Archives: Men’s Health

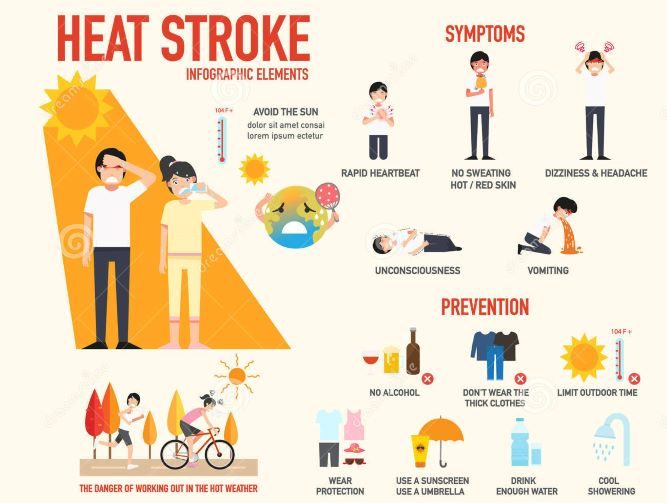
Dr. C’s Journal: Risks & Symptoms Of Heatstroke
We humans, in common with all mammals and birds, are homeothermic; we defend a body temperature of approximately 98.6 F.. When we are cold, we shiver to warm up. If we get too cold, such as being in 50° water temperature for 50 minutes, we have a 50% chance of dying. When we are warm, we sweat . When we get too warm, and our core body temperature rises above a critical point, approximately 105°, we may die.
This article is about HEAT EXHAUSTION, which is very topical, considering the season and the recent “heat dome” in the Pacific Northwest, not to mention global warming.
Our main defense against heat is to sweat. The water in sweat has a very high heat capacity. Changing sweat into water vapor requires a lot of heat, which is gratefully donated by the person who is too hot. Too much water vapor in the air, a high relative humidity, decreases the rate of evaporation, and therefore of Cooling. The critical measurement to warn us of Environmental overheating danger is the WET-BULB THERMOMETER, which is used in tandem with the regular, dry bulb thermometer to calculate the relative humidity.
To give perspective, the wet bulb thermometer reached 77° And the dry bulb thermometer read 116° in the pacific northwest, associated with 118 fatalities. In 2003, when Europe was hit by a heat wave, the wet bulb thermometer reached 82.4°, associated with 30,000 deaths.
When it Feels hot (check the heat index), which is related to both the temperature and the relative humidity, you should start to worry. You should drink extra fluids, wear loose fitting clothes, stay out of the direct sun, avoid sunburn, exercise in the cool of the morning and night, not during the heat of the day, avoid closed vehicles, especially for children, and don’t get sunburned, which decreases the ability of the skin to produce sweat.
Certain groups have more risk, such as very young or old age, the obese, and diabetics. Certain drugs, such as Alcohol, diuretics and beta blockers are factors.
Some typical symptoms are heavy sweating, faintness, dizziness, fatigue, muscle cramps, nausea, and headache. If you are hot, and think you might be experiencing heat exhaustion, you should stop all activity, move to a colder shaded place, and drink cool water or sports drinks.
If you’re caring for somebody, you should worry about confusion, agitation, and other central nervous system symptoms; the brain, together with the heart, kidneys and muscles are very susceptible to overheating.
Rectal temperature is the most reliable, and if it gets to 104°, immediate cooling is necessary, even packing in ice. Don’t bother to use aspirin, since it does not work with heat exhaustion. If coma or seizures develop, and the patient is diagnosed with a heat stroke, the fatality rate and long-term neurological complications are grave.
Please read the excellent article by Joe Craven McGinty in the July 10 Wall Street Journal, or the accompanying mayo clinic article. And stay Cool!
—Dr. C.

DOCTORS PODCAST: MEDICAL & TELEHEALTH NEWS (JULY 10)
A weekly podcast on the latest medical, science and telehealth news.

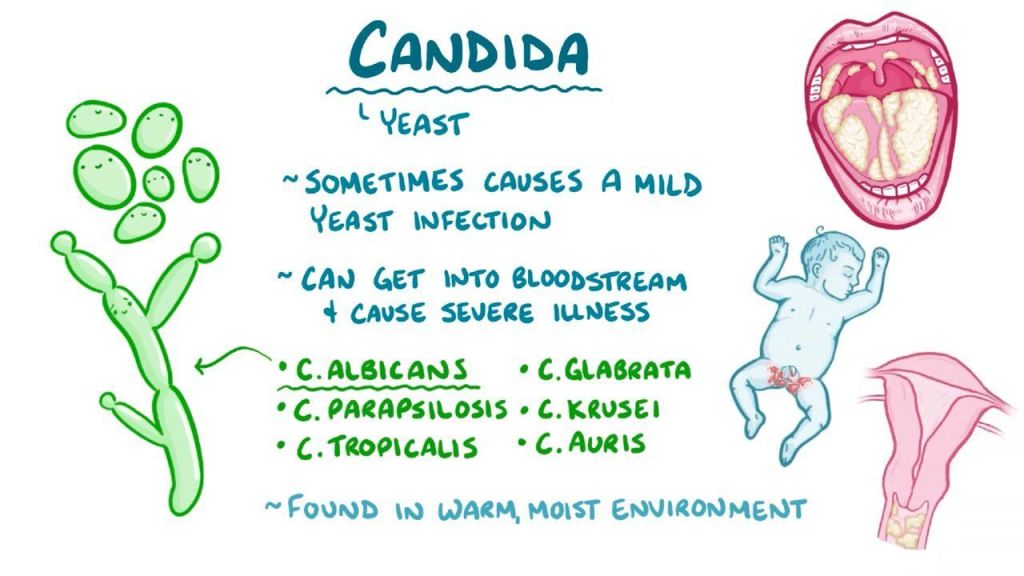
DR. C’S JOURNAL: YEASTS – CANDIDA ALBICANS
Candida albicans is a ubiquitous yeast that has evolved the ability to stick to mucocutaneous linings, e.g. mucous membranes and skin. When present in the mouth it is called thrush, and on the skin intertrigo, or diaper rash among other names.
Almost everybody is infested by candida in low amounts, as indicated by the common incidence of a whitish membrane (thrush) in the mouth of people who regularly use inhaled corticosteroids for asthma. The Cortisone lowers the resistance, enabling the fungus to grow more profusely. The use of broad-spectrum antibiotics also facilitates the growth of Canada by killing off the competition.
Diabetes is a risk factor that commonly increases difficulties that people have in controlling candida growth in their oral and genital areas. Certainly anything that affects the immune system such as very young or very old age, viral infections especially AIDS, organ transplants, and chemotherapy will increase the incidence of Canada.
Due to it’s widespread presence in the body, Candida albicans is the fourth most common cause of bloodstream infections among hospitalized patients, where it grows on indwelling catheters and other in certain devices, which act as avenues for the yeast to invade the bloodstream.
Candida Auris is a member of the same genus, Candida,that has developed some gain of function mutations to allow it to infect the body much more readily. It is very hard to get rid of, and at least one emergency room has been shut down because of a Candida Auris infestation. Another little trick that it has evolved is resistance to most antifungal agents; The mortality rate of systemically infected people is very high.
The combination of greater infectivity and resistance to treatment makes it formidable indeed, but still it is mainly a problem for immuno suppressed individuals. C. Auris is not as widespread as Candida albicans, and the number of cases is currently nowhere near as great. But if you get it, watch out!
As with so many other problems, it is better not see them. In other words, stay healthy with sleep, diet and exercise.
–Dr. C

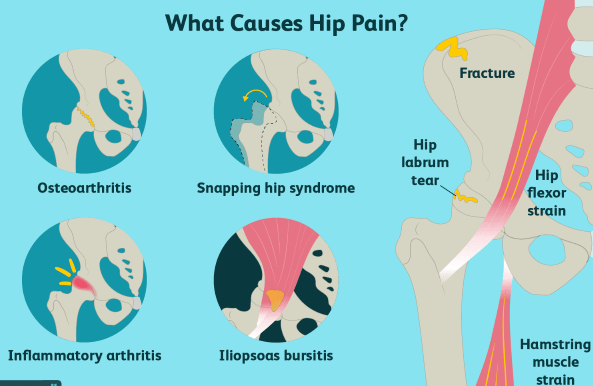
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #42: HIP JOINT PAIN
Hip pain is a very common condition as one gets older, though it can also occur in younger people. The most common cause of hip pain is OSTEOARTHRITIS , a condition that I discussed a little more than a year ago, mainly in the context of pain in the joints of the hand: press the search button and type in “osteoarthritis”. I think you’ll enjoy reading it, as I did upon rereading.
Large joint arthritis seems to be a different animal as compared to small joint arthritis, to which I can personally attest; I have had significant arthritis in the joints of my hand and somewhat in my feet for a long time now, while I am fortunate enough not to have any problem with my hips or knees. It may be a coincidence, but I have been taking glucosamine and chondroitin for sometime now.
It is also of interest that I have stood without sitting down in much of my medical career, and I have continued walking for exercise 1 to 1 1/2 hours a day. This would be against the idea that it is only ordinary wear and tear on the joints that determine the loss of articular cartilage so characteristic of osteoarthritis.
Unusual wear and tear, such as in football, soccer and Long term running on a hard surface, is a different matter, however. Pain in the groin is the most characteristic location for hip-joint arthritis. Pain in the side of the hip joint may be trochanteric bursitis, and that in the buttocks area could be from the nerve root compression of sciatica. Knee pain can refer to the hip. Rheumatoid arthritis, and even rheumatic fever in younger people can also cause hip inflammation and pain.
Sports injuries and falls can cause a hip fracture or a tear in the hip labrum that can declare as pain, but here’s the problem is more about how to treat it, rather than the diagnosis. As you get older, remember to take your calcium and vitamin D to prevent osteoporosis, and maintain your muscle strength and balance to prevent falls. Please type in “falls” for a discussion on how to prevent this often devastating problem in the elderly.
The hip joint can actually get infected with a septic arthritis, which is more typical of younger individuals, and those with immune deficiency. Cancer and infection of the hip bone can also be quite painful. The hip bone can suffer a loss of arterial supply, causing avascular necrosis in the process. Adolescents can get a slipped epiphysis.
When hip pain interferes with your exercise routine and ordinary life activities, it is time to check with the doctor to see what is going on and what can be done about it. If you have not already decided upon surgery, I would suggest a family practitioner or internist as your first stop.
Please refer to the mayo clinic article for more information.
—Dr. C.
Read Mayo Clinic article

HEALTH: HIP REPLACEMENT SURGERY SUCCESS RATES
The mission of COMPASS is to provide patients with access to comprehensive quality and safety data across a variety of Massachusetts General Hospital surgical specialties. In this video, learn about performance data for Mass General hip replacement surgery including its success rate and recovery and rehabilitation.
THE DOCTORS 101 CHRONIC SYMPTOMS & CONDITIONS #41: COCCIDIOIDOMYCOSIS
Coccidioidomycosis, also called Valley Fever, is a silent epidemic in the western hemisphere between 40° north and 40° south. Hot summers and mild winters with an annual rainfall of 10 to 50 cm is typical.
The Fungus grows in the soil that is moist, but the soil must dry out and Be disturbed, such as by digging, and the wind speed must pick up before you can get the arthrospores into the air so that they can be taken into the lungs.
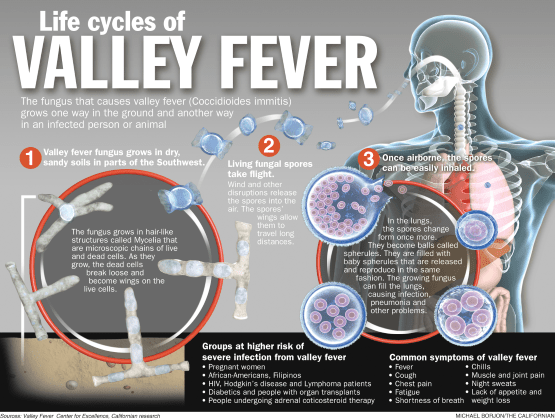
Most infected people have minimal symptoms. Among those infected, some get a fever and a cough and recover promptly. 3 to 5% of individuals develop a chronic infection. Infected patients with a weak immune system can have disseminated coccidiomycosis affecting virtually any tissue in the body.
Notable coccidiomycosis symptoms include a profound feeling of tiredness, fever, cough, headaches, rash, muscle and joint pain. A loss of the sense of smell is also described, raising some confusion with COVID-19.
Coccidiomycosis can cause a characteristic painful bump in front of the lower leg called erythema nodosum. People with a combination fever, joint pain, and erythema nodosum are said to have “desert rheumatism”.
20% of community acquired pneumonia can be due to coccidiomycosis in endemic areas such as Phoenix Arizona and the San Joaquin Valley.
Immunizations have been evaluated for cost-effectiveness, and the results were not encouraging. More recently, A modification of the coccidiomycosis genome which prevents growth and multiplication of the spore has been tried as a vaccine in mice and found effective.
It is planned to try this noninfectious spore on dogs, who are also very susceptible to the disease. Dogs are a good choice because Government restrictions and requirements are not so severe, and because people would do almost anything to protect their animals, promising a good market for the vaccine.
A year ago last spring, my brother had a protracted problem which involves his lungs and even his heart, and was admitted to a hospital in Phoenix. Apparently COVID-19 was ruled out, and Coccidiomycosis was diagnosed. The Doctors declined to give him amphotericin or an Azole, the usual treatments. He recovered, was discharged, and currently is doing well with no residual symptoms.
I was planning to visit him last spring, but I’m glad I stayed home; our immune system‘s are too similar.
–Dr. C

DR. C’S JOURNAL: COPD -CHRONIC OBSTRUCTIVE PULMONARY DISEASE
COPD is the brother of asthma. Both can cause shortness of breath and wheezing. Asthma is the more Treatable of the two, and is due to muscle spasm around the airways which narrow those airways making it more difficult to breathe in and especially out.
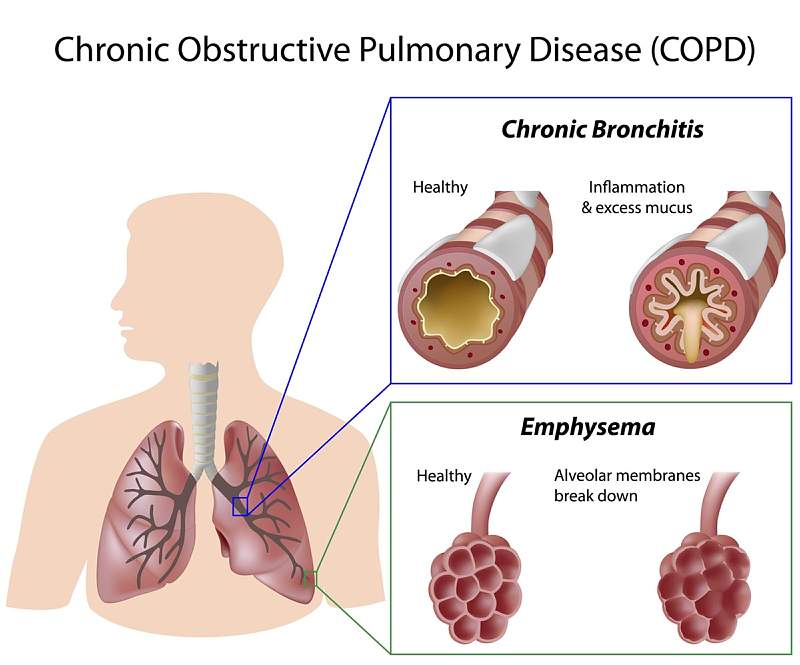
COPD comes in 2 general forms, Chronic bronchitis and emphysema.
Chronic bronchitis is an inflammation of the airways, which differs from the usual allergic asthmatic TH2 type of inflammation. The inflammation of chronic bronchitis is the more common TH1 inflammation that comes from the likes of bacteria and viruses.
The second type of COPD is usually caused by cigarette smoke or other fumes which lead to the destruction of the air sacs and associated elastic tissue, allowing a check valve type of obstruction to occur on breathing out.
COPD is rarely a pure type of chronic bronchitis or emphysema, and is usually an admixture of the two. In fact there can be an “asthmatic element” mixed into COPD, which allows for a better response to the myriads of medication that we now have for asthma.
The symptoms of COPD include shortness of breath, wheezing, chest tightness and chronic cough with production of sputum. Coughing up a significant volume of phlegm from your chest suggests chronic bronchitis rather than emphysema.
The symptoms of COPD come on rather slowly and are usually not noticed until the problem is severe. After all, the cigarette smoker is EXPECTED to cough isn’t he?
As COPD becomes very advanced, fatigue, lack of energy, and unintended weight loss may occur. Swelling of the legs may be a problem and could indicate involvement of a heart; with COPD the right side of the heart has a hard time moving blood through the diseased lungs.
We’ve all seen people pushing around a cart with an oxygen tank. These people most often are smokers who developed COPD. One particularly disgusting advertisement against cigarette smoking showed a person with a hole in the windpipe (tracheostomy) through which he was smoking his cigarette.
Pulmonary function testing it’s often helpful in diagnosing asthma and COPD. In pulmonary function testing, the amount of air in the lungs and the rapidity with which it can be expelled from the Lungs is measured and graphed. it is the rate of flow on exhalation that is diminished in COPD and asthma, the slower the rate the worse the blockage.
In the case of asthma the test is repeated after a bronchodilating adrenaline type medication has been given. The REVERSIBILITY of the airway obstruction is shown by comparing the airway function before and after treatment With no improvement, usually COPD is usually the culprit.
In both asthma and COPD, respiratory infection is a big problem. The compromised lung is usually very vulnerable to these inflammatory reactions. There are a score of medications that are commonly used in asthma which also benefit COPD to a certain degree. Doctors have a large armamentarium for respiratory disease these days.
As mentioned, asthma is more treatable. However if it is poorly treated or neglected, a condition known as REMODELING can occur which will render treatment less effectual.
Please check with the Mayo clinic article on COPD for more information.
—Dr. C.

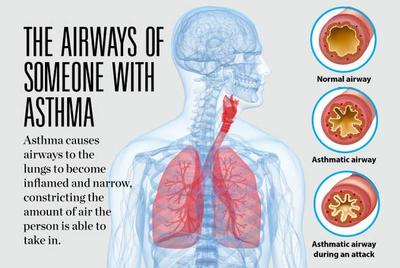
DR. C’S JOURNAL: ASTHMA – DIAGNOSIS & TREATMENT
Asthma is a lung condition with narrowing of the airways, especially on exhalation, or breathing out. This narrowing leads to the musical sound on breathing the air out of the lungs that I heard so often with my stethoscope and over the phone, when I was in active allergy practice. With an asthma attack, the blockage to airflow can become severe enough to dangerously raise the carbon dioxide concentration in the blood stream, and lower the oxygen content.
Many attacks occurred at night .Over the phone, I had older kids and adults take a deep breath, and count from 1 to 30 as rapidly as they could. If they could count out loud to 30 with one breath, at least the obstruction and attendant blood gas changes were not usually serious at that moment in time. That helped me decide whether or not I had to see them in the emergency room.
Asthma is an inflammatory condition of the lining of the airway that stimulates the smooth muscle surrounding the airway to constrict and obstruct flow of air, particularly on exhalation. Early on in my medical practice the main pathology was thought to be overactive airway muscles, and the main effort was to relax those muscles so that breathing could be easier. This was typically done with adrenaline injections, or the inhalation of adrenaline-like agents such as albuterol.
More sustained opening the airway was accomplished by oral theophylline. As time went on, it became known that its effectiveness required a certain blood level. We had an HPLC machine in the office to measure this. 5 to 10 µg per milliliter was required for relief, and anything over 20 µg per milliliter was dangerous. Many cases of convulsions have been recorded in people with excessive blood levels.
We were always aware of the fact that cortisone medications would relieve asthma, but regular use of these drugs caused worrisome side effects such as interference with growth in children, osteoporosis, weight gain and loss of sleep or other problems. Most worrisome was the possibility of adrenal insufficiency and sudden death. We used Cortisone only as a last resort.
There was a group of young children especially 1 to 6 years of age that developed extreme asthma a few days after they developed a common cold. I found that giving prednisolone for two or three days at the start of a runny nose would block the advent of this asthma, without suppressing the adrenal gland. Three days of prednisone was also used to blunt severe attacks.
The excellence of Cortisone in the treatment of asthma should’ve told us that inflammation was a particularly important factor. It is now known that Asthma is not a disease of airway smooth muscle sensitivity per se, but rather a chronic inflammation of the airways that causes the muscles to be irritable.
Asthma is more common in allergic individuals, particularly when they are young. For this reason, the allergies are treated by avoidance of exposure to such things as cats, dogs, house dust and pollen. Allergy injections to the skin test positive items is also useful.
Currently, asthma is treated by inhaling special cortisone preparations and long acting bronchodilators.
The chain of chemical reactions that cause asthmatic airway inflammation has become apparent over the years. Drugs to block these are available, and include special antibodies can be exceptionally expensive; but very effective.
The youngest of my former partners is still practicing Allergy, and almost never has to deal with acute severe asthma.
The beast has been tamed, if not conquered.

