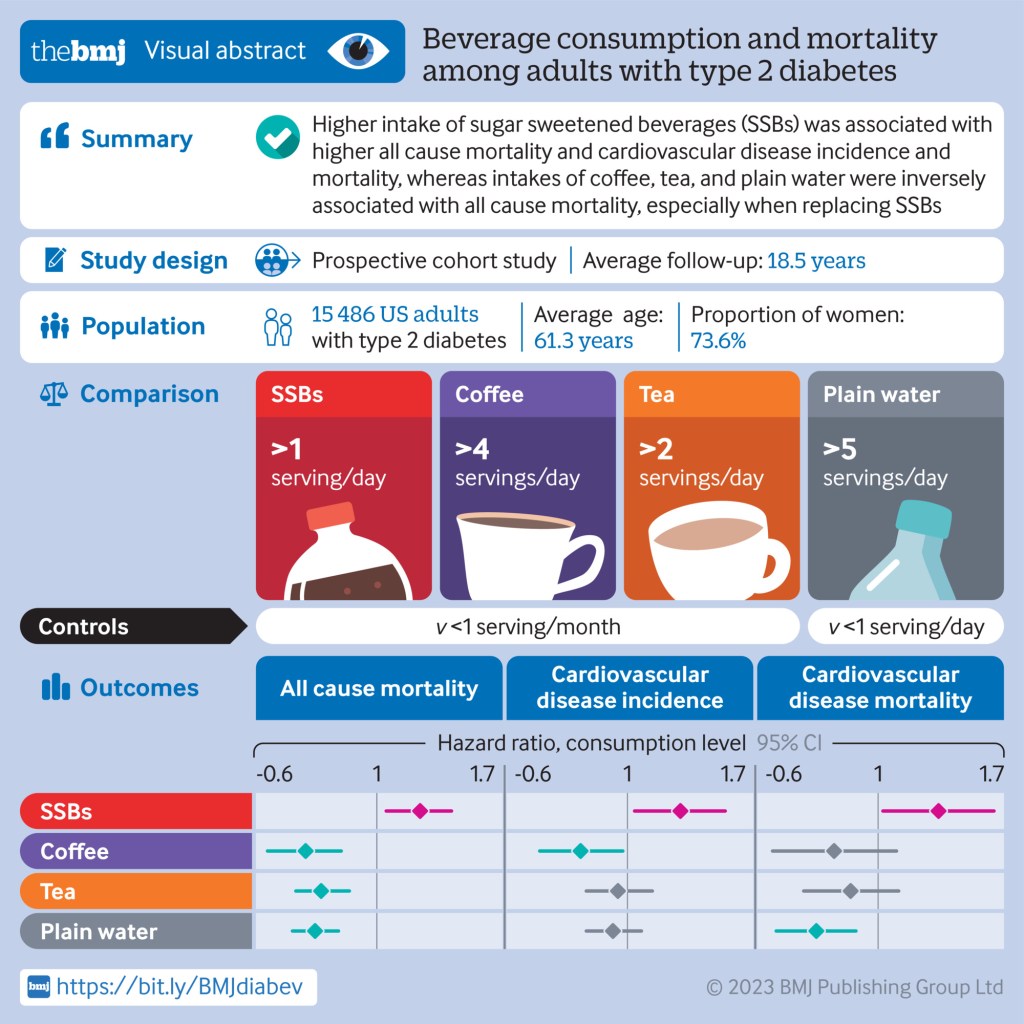
Conclusions: Individual beverages showed divergent associations with all cause mortality and CVD outcomes among adults with type 2 diabetes. Higher intake of SSBs was associated with higher all cause mortality and CVD incidence and mortality, whereas intakes of coffee, tea, plain water, and low fat milk were inversely associated with all cause mortality. These findings emphasize the potential role of healthy choices of beverages in managing the risk of CVD and premature death overall in adults with type 2 diabetes.
NEJM Group (March 29, 2023) – In this Double Take video from the New England Journal of Medicine, Sam Telford and Robert Smith provide a clinical overview of the various tickborne diseases commonly encountered across the United States, including Lyme disease, babesiosis, and anaplasmosis, among others.
Starting with characteristics of ticks and their ability to act as disease vectors, the video reviews the clinical presentation of these infections, clues on physical examination, and laboratory tests to consider when encountering a patient with a potential tickborne infection.
Tick-borne diseases are transmitted through the bite of an infected tick. These include Lyme disease, Anaplasmosis, Ehrlichiosis, Babesiosis, Powassan (POW), Rocky Mountain Spotted Fever, and Tularemia. Ticks can be infected with bacteria, viruses, or parasites.
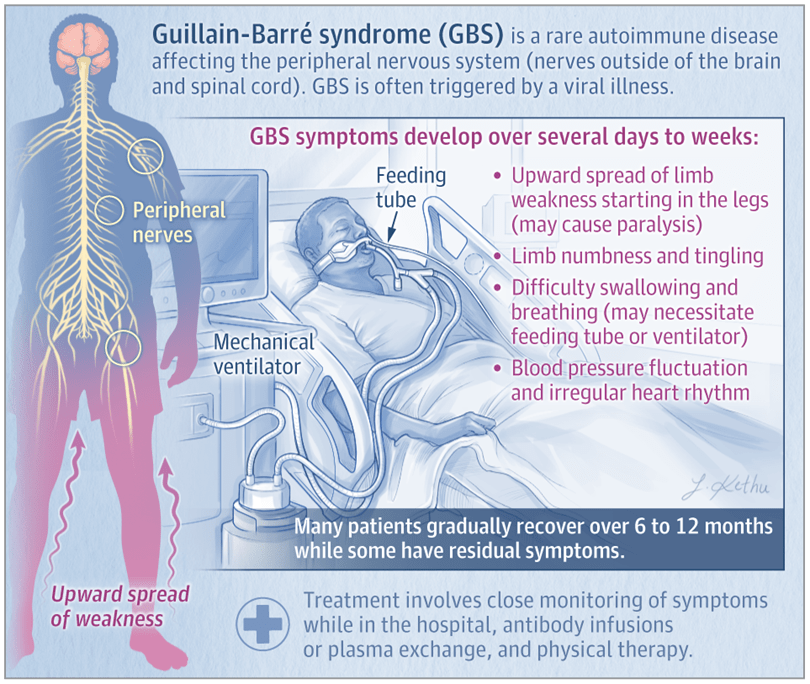
Guillain-Barré syndrome is an autoimmune disease that affects the nerves outside the brain and spinal cord (the peripheral nerves) and develops over several days to weeks. GBS can cause severe muscle weakness, and death occurs in about 5% of patients. The most common subtypes are acute inflammatory demyelinating polyradiculoneuropathy (AIDP) and acute motor axonal neuropathy (AMAN). Approximately 90% of people with GBS in North America and Europe have AIDP.
Signs and Symptoms of GBS
Patients with the AIDP subtype of GBS typically have weakness that starts in the legs and spreads to the arms, as well as decreased or absent reflexes. In more than 50% of these patients, nerves that originate in the brain stem (cranial nerves) are affected, which may cause facial weakness, difficulty swallowing, and eye muscle weakness or paralysis. Approximately 25% to 30% of patients develop severe weakness or paralysis of the muscles used to breathe. GBS commonly causes symptoms of low back pain and limb numbness and tingling, and fluctuations in blood pressure or an irregular heart rhythm can also occur.
Risk Factors and Conditions Associated With GBS
GBS affects people worldwide, and the lifetime risk of GBS is estimated at 1 in 1000. Although individuals of any age can develop GBS, the incidence increases with age, and males are slightly more likely to develop GBS than females.
Approximately two-thirds of patients have a diarrheal or respiratory illness within 4 to 6 weeks prior to the onset of GBS symptoms. Other, less common events or conditions that may trigger GBS include recent surgery, pregnancy, and immunosuppression. Although rare sporadic cases of GBS have been reported after vaccinations, the risk of developing postvaccination GBS is much lower than the risk of developing GBS after an infection.
Diagnosis and Treatment of GBS
Diagnosis of GBS is made based on symptoms and physical examination findings. Neurological testing often includes electromyography and nerve conduction studies to assess nerve and muscle function. Results of a spinal tap (lumbar puncture) may support the diagnosis of GBS and can rule out other neurological diseases.
Individuals with suspected GBS should be admitted to the hospital. All patients with GBS need close monitoring of their breathing, heart rate, and blood pressure. Individuals who develop severe respiratory muscle weakness or paralysis are supported with mechanical ventilation. Patients who have difficulty swallowing may receive nutrition through a feeding tube.
Current recommended treatments for GBS are intravenous immune globulin (IVIG), an infusion of antibodies, or plasma exchange, which involves removal and replacement of the liquid component of blood. About 40% to 50% of patients with GBS do not improve within 4 weeks after IVIG or plasma exchange and need prolonged supportive care. Physical, occupational, and speech therapy are important to help patients regain strength and function.
What Is the Prognosis of GBS?
Most patients with GBS gradually improve and can have a complete recovery over 6 to 12 months. However, some patients have residual symptoms, including fatigue, pain, numbness, tingling, and muscle weakness. Some factors associated with a higher risk of death due to GBS include older age, more severe disease, and need for mechanical ventilation.
Research & review on #Alzheimers, global burden of benign prostatic hyperplasia, #WHO def of vitality capacity, IPD meta on social connection & #cognition, #oralhealth for older people & more.
— Telemedicine Journal (@Telemedicine_Jn) June 10, 2022
What Works Best to Engage Participants in Mobile App Interventions and e-Health: A Scoping Review
Enhancing participant engagement is considered a key priority for wellness and health care, especially as health care undergoes a shift toward the integration of digital technologies (e.g., mobile apps, health care monitors, and online portals with their consumer interfaces).1,2 Technological systems play a critical role in enhancing participant engagement.1,2 Among urban and low-income mothers, the use of smart-device technology for communication was a particularly important contributor to higher retention in longitudinal studies.3 Providing digital health tools has not only led to an increase in study participation adherence rates,4 but it has also contributed to measurable improvements in health care outcomes across several conditions. For instance, greater patient activation in their health care improved patient adherence to treatment prescriptions.5 Participants’ use of web portals to augment treatment of diabetes demonstrated improved glycemic control across multiple studies.6–8 Other studies have seen improvements in participants with HIV,9 with coronary artery disease,10 and with depression,11–13 highlighting how impactful the implementation of these tools can be across different clinical populations.
Schoeppe et al.14 emphasized common strategies that successful mobile interventions often use, such as goal setting, self-monitoring, and performance feedback in their app design. To our knowledge, however, there has not been a scoping review of the specific components of mobile intervention apps that increase engagement. Common across all digital health tools are the focus on increased patient engagement and “empowerment,” which is a result of several qualities inherent in these tools. Most of these technological systems improve patients’ communication with and access to health care providers,1,2,15 and provide patients with more comprehensive information about their health on demand.2,15 While these qualities are common across successful tools and play a large part in improving patient self-management and decreasing stress,2 improved engagement is no guarantee.
Furthermore, measuring engagement is a challenge that has likely contributed to our lack of knowledge on app components that effectively increase this important metric. There are now several measures that quantify the amount of engagement that patients feel toward the digital tools and apps that are being developed,2,15 but these are not widely used and engagement measurements are not standardized across studies. Some examples of such measures are the Patient Activation Measure (PAM16), Mobile App Rating Scale (MARS17), and the Patient Health Engagement scale (PHE-s18). These measures create a quantifiable standardized method by which researchers can measure the phenomenon of user engagement during program development, and are important considerations when creating new digital tools for patients and clinical research participants.
Empowering Patients Through Education And Telemedicine